 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
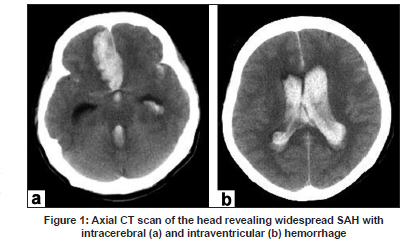
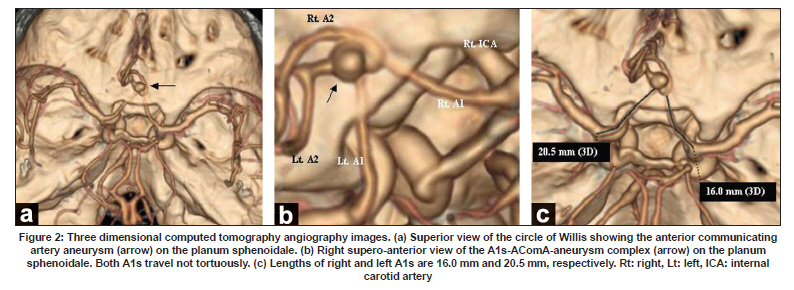
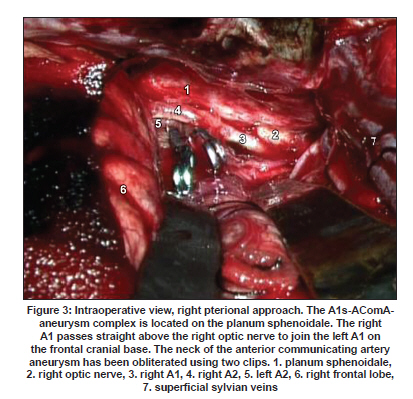
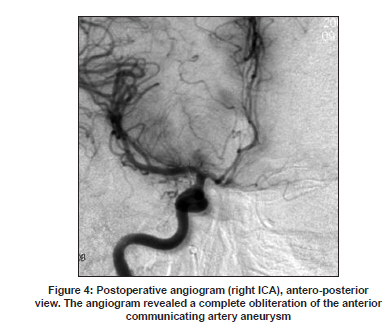
Neurology India, Vol. 57, No. 6, November-December, 2009, pp. 831-832 Letter To Editor An unusual variant of the ruptured anterior communicating artery aneurysm located on the planum sphenoidale Masatou Kawashima, Takao Kitahara1 , Kazui Soma1 , Kiyotaka Fujii Departments of Neurosurgery and 1 Emergency and Critical Care Medicine, Kitasato University, School of Medicine, Sagamihara, Kanagawa, 228-8555, Japan. Date of Acceptance: 08-Jan-2009 Code Number: ni09241 PMID: 20139534 DOI: 10.4103/0028-3886.59501 Sir, The anatomy of the anterior cerebral artery (ACA) is highly variable and the variations in the anterior communicating artery (AComA) complex are quite common and are well described. [1],[2] We describe an unusual variant of AComA aneurysm located on the planum sphenoidale. A 51-year-old previously healthy woman was admitted with a sudden onset of headache. On examination the grade of subarchnoid hemorrhage (SAH) was Grade V (World Federation of Neurological Surgeons). The initial computerized tomography scan revealed widespread SAH with right frontal intracerebral and intraventricular hemorrhage [Figure - 1]a and b. Three dimensional computed tomography angiography (3D-CTA) revealed an aneurysm located at the AComA complex on the planum sphenoidale. Both A1s had a course to the planum sphenoidale over the tuberculum sellae to join the AComA [Figure - 2]a and b. The length of the left and right A1s were 20.5 and 16.0 mm, respectively [Figure - 2]c. No other aneurysms were identified. Surgical clipping of the aneurysm through the right pterional approach was performed without complication. The aneurysm was located on the planum sphenoidale, but was not adhered to the frontal skull base [Figure - 3]. The postoperative angiogram revealed a complete obliteration of the aneurysm [Figure - 4]. The patient underwent the ventricular-peritoneal shunt for the hydrocephalus developed two months after the initial SAH. Patient was left with severe disability because of the initial SAH. Morphological variantions of ACA, including duplicate A1, duplicate or multichanneled AComA, and failure of pairing of the distal ACA have been frequently reported. [1],[2],[3],[4],[5],[6] However, variations in the location of the AComA complex have not been well document in the literature. In the cases of intrasellar aneurysms originating from the AcomA, [7],[8] AComAs were located above the chiasm or optic nerves. The A1 courses above the optic chiasm or nerves to join the AComA. The junction of the AComA with the right and left A1 is usually above the chiasm (70% of brains) rather than above the optic nerves (30%). [1],[2] Of the arteries traversing above the optic nerves, most traverse above the nerve near the chiasm rather than distally. The arteries with a more forward course are often tortuous and elongated and some of them rest on the tuberculum sellae or planum sphenoidale. The length of A1 varies from 7.2 to 18.0 mm (average, 12.7 mm). [1],[2] In the present case, the course of both the A1s were not tortuous, but were rather straight. The left A1 was 20.5 mm in length, which is probably the longest length ever reported. Preoperative recognition of the location of the aneurysm in our patients helped us to clip the aneurysm without much of intraoperative problems. 3D-CTA is superior imaging modality to magnetic resonance angiography (MRA) and conventional angiography in understanding the relationship between the aneurysm and surrounding structures in spite of the bony artifacts. [9] The AComA aneurysm located on the planum sphenoidale is quite unique. To our knowledge, this AComA aneurysm variant has not been previously described. The importance of recognizing this variant is related to the planning of surgery in the AComA region. References
Copyright 2009 - Neurology India The following images related to this document are available:Photo images[ni09241f2.jpg] [ni09241f4.jpg] [ni09241f1.jpg] [ni09241f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}