 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
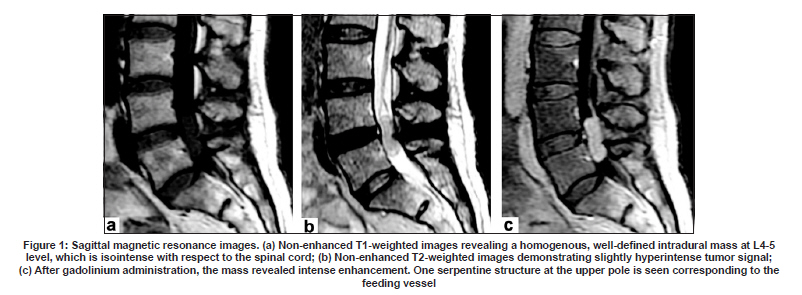
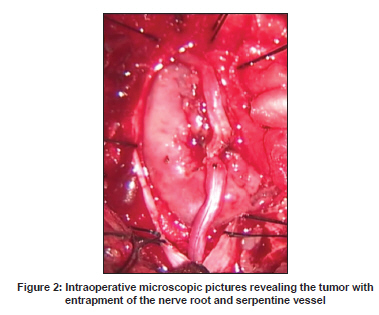
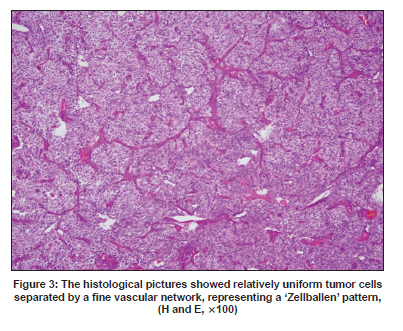
Neurology India, Vol. 57, No. 6, November-December, 2009, pp. 833-834 Neuroimage Paraganglioma of the cauda equina Cheng-Ta Hsieh, Wen-Chiuan Tsai 1 , Chi-Tun Tang, Ming-Ying Liu Departments of Neurological Surgery, 1 Pathology, Tri-Service General Hospital, National Defense Medical Center, Taipei, Taiwan, Republic of China Date of Acceptance: 11-Mar-2009 Code Number: ni09242 PMID: 20139535 DOI: 10.4103/0028-3886.59502 A 48-year-old female presented with symptoms of low back pain and radiation down the posterior aspect of both the legs of six months duration. She was not a known case of diabetes and hypertension. On admission, physical examination was unremarkable. The neurological examination revealed sensory deficits in the distribution of L4 and L5 dermatomes on both the legs. The muscle power was normal and tendon reflexes were normal. The plain X-ray of lumbar spine was normal. Magnetic resonance imaging (MRI) showed an intrathecal extramedullary well-defined tumor measuring about 2.5 x 0.7 x 1.2 in size at the level of L4-5. The tumor appeared as isointensity with respect to the spinal cord on T1-weighted sequences and hyperintensity on T2-weighted image [Figure - 1]a and b. Contrast MRI showed homogenous enhancement of the tumor and also a serpiginous enhancing vascular structure extending from conus medullaris to the tumor [Figure - 1]c. She underwent L4 and L5 laminectomy to remove the tumor. At operation the tumor was soft and reddish and was attached to one of the nerve roots. A single vessel along the nerve root was found entrapped into the tumor [Figure - 2]. Histopahtological examination shwed, nests of tumor cells separated by a fine vascular network, representing a 'Zellballen' pattern [Figure - 3]. Immunohistochemical staining was negative for glial fibrilary acid protein and was positive for synaptophysin and chromogranin A. In addition, the expression of S-100 showed the existence of sustentacular cells. Pathological studies confirmed the diagnosis of paraganglioma. Paragangliomas, derived embryologically from the autonomic system, commonly arise in the adrenal medulla, pheochromocytoma. [1] Paragangliomas of the central nervous system are very rare and about 200 cases of paragangliomas of cauda equina have been reported in the literature till date. [1],[2],[3] There was male gender preponderance and the mean age at presentation was 45.9 years. Lower back pain and radicular pains were the most common symptoms. As paragangliomas of cauada equina is rare, these tumors are often mistaken preoperatively for forepdenamyomas or schwannomas. [4] MRI is considered to be the imaging modality of choice.to differentiate the intrathecal tumor. The MRI characteristics of paraganglioma of cauda equine have been well studied. [1],[2],[4],[5] Typically paraganglioma appear isointense to the conus medullaris on T1-weighted sequences and hyperintense on T2-weighted sequences, as seen in our case. Sometimes, heterogeneity on T2-weighted sequences may be seen and it is due to subacute or chronic hemorrhage. Because of a high vascularity paragangliomas show remarkable heterogenous enhancement with gadolinium injection. The other typical finding is "serpentine flow voids" extending from the tumor to the conus medullaris. This finding is attributed to the tumor hypervascularity or the congested veins. [5] The detection of the typical serpentine structure has been considered as diagnostic of paragangliomas. Our patient showed the typical features of paraganglioma of cauda equina on MRI, especially 'the serpentine sign'. This sign was confirmed by the findings at operation. Probably ours is the first such demonstration at operation. Total surgical excision is the best option to achieve greater chance of cure and also the option to reduce the recurrences. [3] References
Copyright 2009 - Neurology India The following images related to this document are available:Photo images[ni09242f3.jpg] [ni09242f2.jpg] [ni09242f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}