 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 58, No. 1, January-February, 2010, pp. 6-14 Review Article Congenital Chiari malformations: A review Prasad Vannemreddy, Ali Nourbakhsh, Brian Willis, Bharat Guthikonda Department of Neurosurgery, LSU Health Sciences Center, Shreveport, USA Correspondence Address: Dr. Prasad Vannemreddy, Department of Neurosurgery, University of Illinois at Chicago. 912 S Wood street, M/C 799, Chicago, IL 60612, USA, prasad4458@hotmail.com Date of Acceptance: 17-Aug-2009
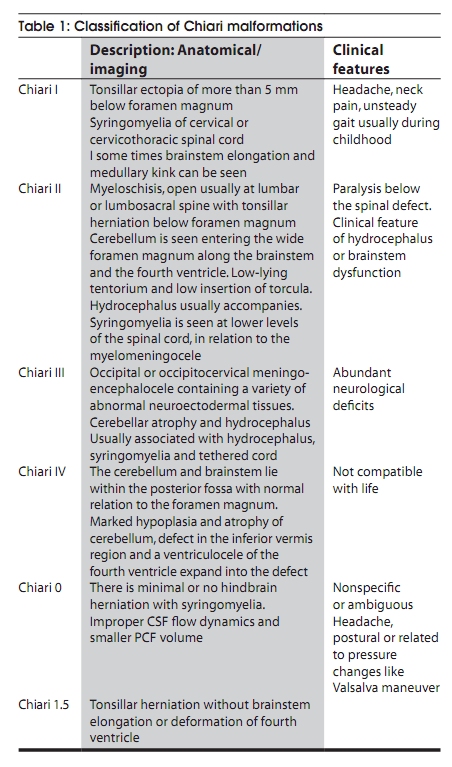
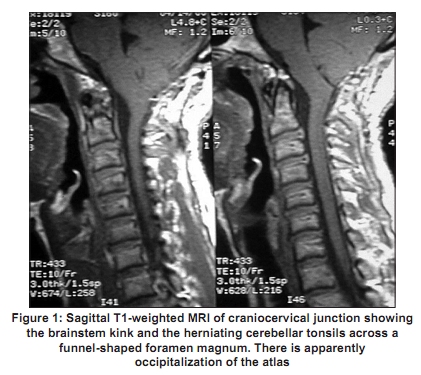
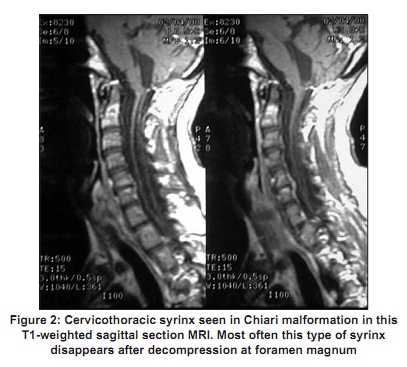
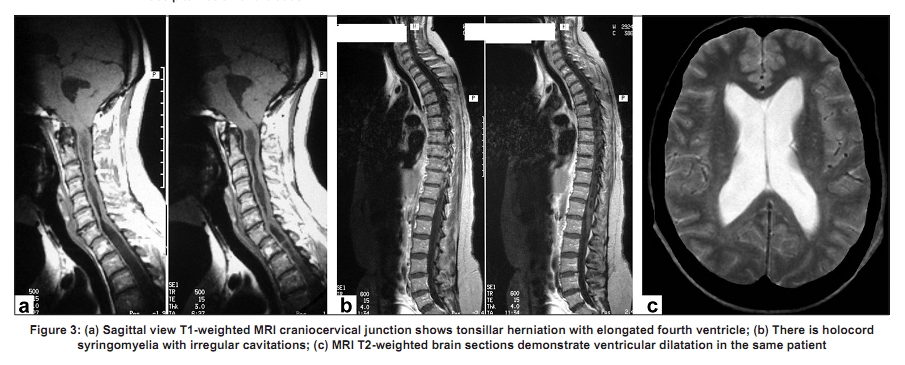
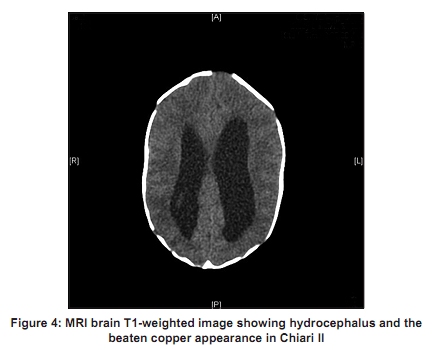
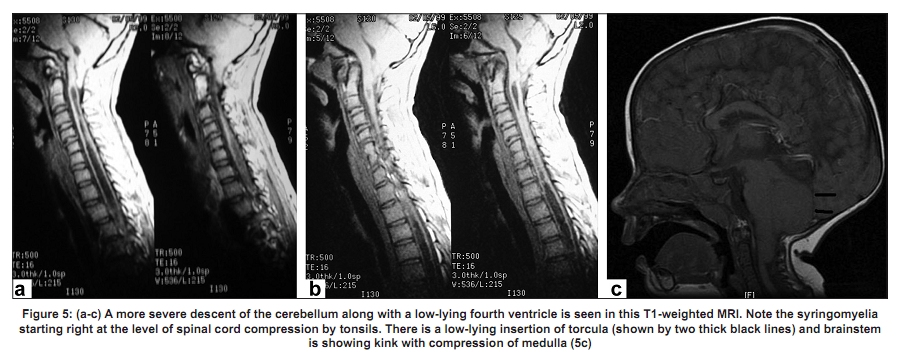
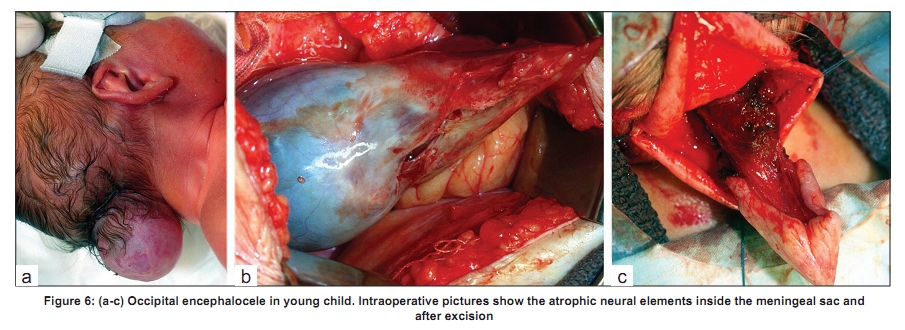
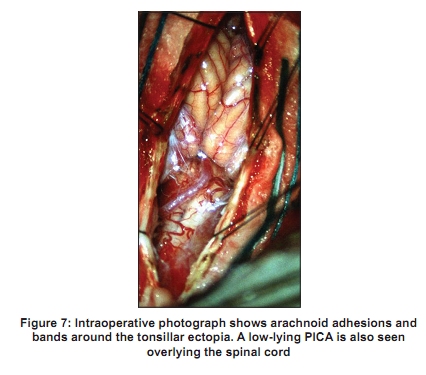
Code Number: ni10003 DOI: 10.4103/0028-3886.60387 Abstract Chiari malformation is the commonest anomaly of the craniovertebral junction involving both the skeletal as well as the neural structures. This entity has rapidly evolved over the past decade with newer visualization techniques, thus posing new challenges to diagnosis and management. This review includes the developmental theories, the latest nomenclature and existing treatment modalities of this interesting anomaly. Five theories tried to explain the malformation of the hindbrain and the neuraxis but no single theory completes the development of embryonic defects. Several atypical presentations have been reported with either incidental/asymptomatic features resulting in further classifications. The new magnetic resonance imaging flow techniques attempt to substantiate the clinical presentations and correlate with the abnormality which can be subtle in correlation. Surgical correction to improve the cranial volume, decrease the hydrocephalus and improve flow across the foramen magnum is the mainstay but needs to be tailored to a given type of malformation. Further clinical and imageological studies, especially longitudinal natural history, might improve our understanding of the atypical/asymptomatic presentations and the management that is currently available.Keywords: Anomaly, Chiari malformations, congenital, craniovertebral junction, syringomyelia Inroduction A complex range of anomalies of the hindbrain formation appearing at various stages of growth and development of the central nervous system (CNS) are included under this group called Chiari malformations (CM). John Cleland described a case of hindbrain malformation at autopsy in 1883. Hans Chiari, an Austrian pathologist, published a detailed description of hindbrain malformations following postmortem examinations of 40 cases in 1891 and again in 1896. [1] During this time, Julius Arnold from Germany also described a single patient with myelodysplasia with associated herniation of the hindbrain. In his initial description, Chiari classified the hindbrain malformations into Types I, II and III and then in his latter publication added the Type IV malformation [Table - 1]. Embryonal Substrate The embryologic timing of the occurrence of the CM is not clear. These anatomic variations could have their origin in the failure of the pontine flexure to form normally from the 28 th to 29 th day of gestation, leading to formation of elongated brainstem. The normal growth of the cerebellum during the third month leads to the caudal vermis and choroid plexus getting under the tonsils. A failure of this process can lead to persistent extraventricular position of the vermis and choroid plexus seen in the malformations. These structural deformities may lead to disturbance of cerebrospinal fluid circulation and produce an embryonic hydrocephalus. The secondary hydrocephalus could lead to further herniation of cerebellar tissue into the spinal canal and also drag the tentorium downwards, thus reducing the posterior fossa dimensions. [2] Many genetic and environmental factors might play a role and five different theories have been considered in explaining the embryogenesis. [3] Embryology and Pathogenesis of Chiari Malformation Developmental arrest Myeloschisis is described as a result of failure of closure of the neural tube due to arrested development with subsequent secondary events. [4] Daniel and Strich proposed developmental arrest as a possible cause of CM, especially in the progression of pontine flexure during days 28 and 29 (Stages 13 to 16). [5] Marin-Padilla and Marin-Padilla induced mesodermal insufficiency in hamsters by vitamin A that led to underdevelopment of occipital somites and thus a shallow posterior fossa. This theory fails to explain many other observations like smaller cerebellum making a shallow posterior fossa as a secondary phenomenon [6],[7] and the existence of malformation during 16-18 weeks gestation. The flattening of the skull base may be a secondary occurrence in the second half of gestation according to human embryo studies. [6] Overgrowth This theory suggests that the neural plate overgrows prior to neurulation preventing fusion of neural folds. [8] In 1883, Cleland accepted this theory to explain some forms of spina bifida. Barry et al., reported increased volume of cerebellum and brainstem in two human fetuses of 17 and 18 weeks of development with evidence of CM. [9] However, no other work supported this observation and the cerebellum in infants with CM weighs uniformly less than normal at all ages. [10],[11] Hydrodynamic Mechanisms In "The Dysraphic States from Syringomyelia to Anencephaly" Gardner details the works of Morgagni and Chiari who also utilized the hydrodynamic theory to explain all dysraphic states. This was done through a series of mechanical steps consequent to inadequate escape of fluid from the neural tube during the embryonic period or from the subarachnoid space at a later stage. Gardner suggested that a physiologic hydrocephalus exists in the embryo during 43 and 44 days of gestation. According to this hydrodynamic theory, CM results from imbalances between pulsating choroid plexus in the fourth and the lateral ventricles. However, developmentally, fetal myeloschisis appears even before the evidence of choroid plexus formation. Furthermore, fetal hydrocephalus has not been observed in embryos with myeloschisis. [7],[9] Neuroschisis Based on observations in monkey and human embryos, Padget postulated that a closed neural tube reopens to produce spinal dysraphism. [12],[13] A neuroschistic bleb was proposed by Padget which develops from a cleft in the dorsal midline of the closed neural tube, permitting the proteinaceous material to escape into the surrounding mesoderm and elevating the overlying ectoderm. Neuroectodermal-mesodermal spatial dyssynchrony Jennings et al., postulated that the normal zone of fusion at third and fourth somites is displaced caudally below the third to fifth somite pairs thus displacing the area of formation of the cervicomedullary junction. [6] This is supposed to be similar to Daniel and Strich′s theory. [5] Traction theory Traction due to the fixation of the spinal cord to the skin at a lower level prevented upward migration during early development while the cerebellum and brainstem are pulled down as the vertebral column grows. [14] Classification of Chiari malformation Detailed evaluations using current imaging methods have introduced more subtle forms of the malformation currently named as Chiari 0 and Chiari 1.5. Also introduced are terms like "asymptomatic" and "incidental" CM depending upon the extent of cerebellar ectopia and clinical findings. Chiari O The case of differential pressures exerting influence across the cervicomedullary junction is exemplified by presentation of a certain group of people with minimal or no hindbrain herniation and syringomyelia. [15],[16] Many of them show craniocervical abnormalities of Type I and at surgery reveal arachnoid adhesions and bands with crowded foramen magnum. Further support to the theory of improper dynamics of CSF is afforded by a recent study, calculating the volume of CSF in the posterior cranial fossa (PCF). Milhorat et al., reported that some of the ambiguous and nonspecific symptoms of certain people are related to the CSF flow dynamics. [17] As the newly formed CSF gets displaced into the cranial and spinal compartments from the compressed PCF, the compliance of CSF and the damping effect of an open CSF compartment are altered. This produces changes in venous pressures of normal activities like cardiorespiratory excursions/Valsalva maneuvers and posture. Such altered CSF flow dynamics might result in nonspecific clinical features like suboccipital headaches, pseudotumor-like episodes of visual phenomena. Chiari I This is the most common clinical entity and is described as synonymous with tonsillar herniation. This feature is seen in a wide variety of congenital and acquired disorders and radiological definition is limited to tonsillar ectopia of 5 mm below the foramen magnum without any reference to syringomyelia. Based on magnetic resonance imaging (MRI) findings of syringomyelia, Pillay et al., introduced Type A and Type B classification of CM. [18] Bony anomalies While 50% of Chiari I present with basilar and craniovertebral anomalies, [19] De Barros reported 22/66 individuals with Chiari I showing basilar invagination. [20] Zingesser reported 25% of patients with occipitalized atlas having Chiari I. [21] A Mayo clinic report disclosed that 19/60 adults with CM, had craniovertebral junction anomaly. [22] Abnormalities of the fourth occipital sclerotome appear to be closely related to hindbrain malformation, which has led to the strengthening of the theory of mesodermal disorder. [17],[23] Other commonly seen osseous lesions include platybasia, midline occipital keels, remnants of proatlas, atlantoaxial dislocations, Klippel-Feil anomaly, empty sella and clival concavity. [23],[24],[25] Brain and spinal cord It is uncommon to see significant abnormalities of the brain. An occasional patient might show an elongated brainstem with medullary kinking [Figure - 1]. The herniated tonsils appear smooth and atrophic with peg-like appearance. Hydrocephalus is reported in 3-10% of these patients, [26] while fourth ventricle may appear relatively elongated with reduced CSF flow both anterior and posterior to the brainstem. [27],[28] A more frequent observation is syringomyelia, reported in 50-75% of cases. [17],[18],[29],[30] Syrinx cavities are usually found in the cervicothoracic spinal cord [Figure - 2], occasionally with holocord and hydrocephalus [Figure - 3]a-c. Chiari 1.5 An interesting nomenclature introduced by Iskander and Oakes to specifically address patients with tonsillar herniation but without brainstem elongation or fourth ventricle deformation. [31] Chiari II The next grade in severity presents with caudal descent of the cerebellar vermis along with the brainstem and fourth ventricle. This also has a number of associated anomalies, which occur in conjunction with other pathological conditions. Almost all cases of myelomeningocele present with Chiari II though the reverse is not true all the time. [32] Bony anomalies The skull shows signs of intracranial hypertension in the form of beaten copper appearance [Figure - 4]. Scalloping of frontal bones, petrous apex and jugular tubercles is described. Enlarged foramen magnum signifies impact of the PCF due to reduced volume. The upper cervical spine shows Klippel-Feil anomaly with hypoplastic posterior arch of C1 and scalloped dens. [33] CSF compartments Hydrocephalus is seen in 90% of the cases and ventricles are seen asymmetrical; both right to left and frontal to occipital. [34] The fourth ventricle is small and deformed with absent foramen of Magendie. Additional cysts and widened CSF spaces around the brainstem and cerebellum are seen. The vast majority of Type II exhibit syringohydromyelia, sometimes with exophytic components mimicking arachnoid cyst [31],[35] [Figure - 5]a-c. Brain and spinal cord Approximately 6% of cases show spilt cord malformation. [36] Partial or complete agenesis of the corpus callosum with absent septum pellucidum, polygyria, prominent anterior commissure, obliterated longitudinal fissure between parietal and occipital lobes, dysgenesis of olfactory tract/bulb, absent cingulate gyrus and heterotopic gray matter are frequently seen. [37] The midbrain is elongated with a shortened quadrigeminal plate. Peaking is seen with fusion of colliculi (tectal beaking). There may be stenosis of aqueduct, with kinks and compressions. There is gross atrophy of the cerebellum and vermis is seen herniating through the foramen magnum. Pons also looks elongated and flat with dysplastic cranial nerve nuclei. The medulla exhibits the typical kinking that is frequently seen in symptomatic children. [33],[38] Chiari III A single case was described by Chiari and still this remains as a rarely identified entity, characterized by an occipital or cervical encephalocele along with the intracranial abnormalities seen with Type II malformation and a wide foramen magnum. [39] The sac of encephalocele contains dysmorphic and ischemic neural elements [Figure - 6]a-c. Chiari IV This is characterized by marked cerebellar hypoplasia or aplasia and tentorial hypoplasia. There is no hindbrain herniation. Clinical Presentation The prevalence of symptomatic Chiari I malformation is 1 per 1000 in the general population. [40] As the imaging modalities improved the diagnostic abilities, several atypical, silent or incidental entities have been reported. Type I malformations The presentation in early childhood differs from the clinical features observed in the adult patient population. Children younger than three years present with an overwhelming proportion of impaired oropharyngeal dysfunction. In their series Greenlee et al., reported oropharyngeal complaints (aspiration, regurgitation, choking, dysphagia, abnormal vocal cord function, chronic cough) to be the major presentation in children younger than three years of age while the others (>3 years) presented with headache and scoliosis. [41] Other complaints included headache or neck pain worsening with Valsalva maneuvers (42%), sleep apnea or snorting (29%), motor weakness or gait impairment (26%), sensory disturbances (13%), recurrent respiratory infections (13%) and developmental delay (16%). Children presented with pain as a chief complaint (63%) even in the other large series by Park et al., [30] others were numbness (26%), motor weakness (19%) and incoordination (16%). However, 16% were neurologically asymptomatic while 56% had no detectable neurological deficits. In a group of adolescents, 91% presented with pain, 27% had scoliosis. [42] In a large series of adult patients, 81% presented with suboccipital headache, distinctively worsening on physical exertion and Valsalva maneuvers, head dependency and posture changes. [17] Common misdiagnoses included migraine, fibromyalgia and multiple sclerosis. Trauma was a precipitating event in 24% of cases. Type II malformations Almost all cases of myelomeningocele show some features of Chiari II. Typically, the child undergoes repair of the spinal defect, followed by shunt placement for progressive hydrocephalus and subsequent imaging studies disclose the hindbrain anomalies that would constitute the leading cause of death. The above presentation of lower cranial nerve deficits, cerebellar dysfunction and respiratory difficulties are seen with increasing severity in Chiari II while respiratory insufficiency and apnea contribute to mortality. [31] Progressive tethering and/or formation of syrinx usually starting from the site of myelomeningocele repair produce progressive neurological deficits in this group. Type III malformations Chiari III malformations are the rarest form of hindbrain deformities characterized by occipital and/or cervical encephalocele. These children present with severe neurologic deficits including delayed milestones, seizures, ataxia, spasticity and other features common to Type I and II. They are seldom reported, given the rarity; only two among 312 cases of CM had Type III. [43],[44] Diagnostic Imaging MR imaging and its advanced techniques utilizing different sequences coupled with flow studies and cine mode imaging have improved our understanding of CM. [18],[28],[45],[46] Chiari I malformations Chiari I malformation is the most extensively studied entity. Aboulezz et al., studied retrospective data on 95 cases based on clinical examination at the time of imaging and compared with normal population. [47] They considered any descent of more than 5 mm to be abnormal. Barkovich et al., studied normal population and Type I malformations to conclude that 2 mm descent is the normal limit. [48] Normal physiological limit of 6 mm during the first 10 years of age was reported by Mikulis et al., and gradual ascent of tonsils was noted as normal. [49] Irrespective of shorter descent of tonsils, clinical presentation would also depend upon the volume of posterior fossa. Badie et al., determined that patients with small volume of PCF become symptomatic more often than those with normal values and this group of patients respond to surgical treatment in the form of posterior fossa decompression better. [50] A shallow PCF might be preceding hindbrain malformation in certain conditions like craniosynostosis, Paget′s disease, hyperphosphatemic rickets achondroplasia and acromegaly. [51],[52],[53],[54] The most common findings on MRI include compression of CSF spaces posterior and lateral to the cerebellum, tonsillar herniation of at least 5 mm, reduced height of the supraocciput and increased slope of tentorium. [17] Tonsillar herniation of at least 5 mm can be seen as an independent finding incidentally among asymptomatic patients; [55] whereas, Milhorat et al., encountered 9% (32 of 364) of patients with less than 5 mm tonsillar herniation presenting with typical features of Chiari I malformation. [17] All of them had shown MRI evidence of hindbrain overcrowding and CINE-MRI demonstrated abnormalities of CSF flow. Flow obstruction, decreased velocities, shorter duration of flow and preferential cranial flow in cases with more than 5 mm tonsillar herniation are reported. [45] The bulk flow remains normal but marked heterogeneity appears at the foramen magnum in the form of increased cephalad and caudad peak velocities, spatial inhomogeneity, and simultaneous bidirectional flow. All these heterogeneous flow appearances decreased following decompression of PCF. [27] Chiari II malformations The abnormalities along the entire neuraxis are preferably demonstrated by MRI. Hindbrain herniation, caudal descent of fourth ventricle and brainstem and other associated defects are seen with MRI while in utero diagnosis can be performed by ultrasonography. [56] Due to the common occurrence of syrinx at the lower end of the spinal cord, it is preferable to visualize the entire spinal cord. Chiari 0 malformation This new entity is being studied with increasing interest since atypical presentation and absence of tonsillar herniation in cases symptomatic for Chiari I malformations have been observed clinically. MR evaluation of this group of patients demonstrated that the contents of the posterior fossa are compromised and distorted in patients with syringohydromyelia without tonsillar herniation. [16] Surgical Treatment and Outcome Most theories concerning genesis of CMs focus on neurectoderm. However, clinical findings, radiological observations and operative visualization of the posterior fossa from time to time have brought out more of the mesodermal abnormalities in the form of small PCF, defective occipital bone, anomalies of atlas and cervical spine. Other abnormalities are dural bands, arachnoidal adhesions and soft tissue encroachment around the foramen magnum. The more sinister defects like ectopic tonsils, and patent obex received attention in the earlier days but do not seem to require corrective operative measures in the present-day scenario. As a result, most surgeons perform corrective surgery on PCF with augmentation duraplasty and reconstitution of CSF pathways. Chiari I malformations American Association of Neurologic Surgeons has a consensus for conservative surgery for asymptomatic Chiari I. Periodic neurologic examinations with imaging evaluations were favored by the majority. On the other hand, surgical intervention was favored by all for the symptomatic group. A similar strategy was put forth for cases of syringomyelia with imageological progression without clinical worsening. [57] The current practice involves PCF bony decompression including foramen magnum and upper cervical spine, followed by augmentation duraplasty facilitating CSF flow. In brief, a small suboccipital craniectomy is performed, exposing the dura and the occipital venous sinus while excision of the posterior arch of C1 facilitates the dural exposure. The dura is opened vertically in midline, preferably under magnification and tacked laterally to the muscles. Very often, dural bands opposite C1, thickened arachnoid membrane and septations bridging the cerebellar tonsils are seen in the midline. The tonsils are usually tongue-like and smooth, very often pulling down the posterior inferior cerebellar artery along with them into the spinal canal [Figure - 7]. Pericranium from the occipital region or other dural substitute can be used to perform duraplasty. In many centers, the procedure has yielded good results with zero mortality. [29],[58] Postoperative MRI established the efficacy of this method in providing patent CSF pathways around the craniocervical junction. [59],[60] Park et al., had improvement in all the cases over long-term follow-up. [30] Klekamp et al., reported 87% decrease in the size of syrinx in their series of 131 patients [61] while Garcia-Uria et al., had 50% improvement and 75% stabilization over a follow-up period of five and ten years respectively. [62] Fischer reported resolution of syrinx in 93% cases on a literature survey. [63] Anderson et al., reported postoperative improvement in brainstem auditory evoked potentials following craniocervical decompression. [42] Not only do syringomyelia and symptoms of hindbrain compression improve, but scoliosis seen with long segment syringomyelia, also responds to PCF decompressive surgery. [64],[65] Some modifications: Park et al., coagulated cerebellar tonsils to shrink the size and improve the volume of PCF with reduced pressure on the cervico-medullary junction. [30] Krieger et al., left the dura open and did not attempt intradural dissection or lysis of arachnoid adhesions to reduce blood pooling and foreign body reaction around the closure. [66] Chiari II malformations The changes due to brainstem deformity do not show improvements with surgical correction or shunting of hydrocephalus and thus tend to produce progressive neurological worsening. However, the standard procedure includes repair of the myelomeningocele and treatment of hydrocephalus by placing a shunt tube. Periodic evaluations for brainstem malfunction need to be performed, especially for respiratory function, swallowing and speech. If progressive brainstem compression is clinically evident, posterior fossa decompression is indicated. Extensive bone removal is not usually indicated in view of wide foramen magnum and abnormal venous sinuses. After midline durotomy, the arachnoid adhesions need to be lysed and cerebellar vermis is released from compressing the cervico-medullary junction. Foramen Magendie is carefully dissected free of the adhesions and CSF pathways are opened up. Tulipan et al., demonstrated reduction in the extent of hindbrain anomalies, when intrauterine repair of myelomeningocele is performed. [67] Theoretically this repair reduces the fluid loss and thus the hindbrain herniation. Chiari III malformations Given the rarity of these lesions, the natural history of Chiari III malformations remains unknown. Among 312 cases of CM, only two cases were reported to have Type III. [68] Most of these malformations may not be compatible with life, [69] yet surgical repair should still be offered. [70] The repair of the malformation follows the same principles as applicable to open neural tube defects. However, caution is required during repair to avoid damage to brainstem or compression during repair. [71],[72] Shunting of the ventricular system was proposed to reduce the tension in PCF, but clinically had no significant benefit. [73] Chiari 0 malformation Recent cine-MRI and/or flow/velocity studies are helpful to demonstrate CSF flow abnormalities. Cases with syringomyelia presenting with symptoms of posterior fossa compression can be evaluated by this imaging. Oakes et al., have demonstrated the indications and operative results in this group of patients [16] and Milhorat et al., observed similar trends. [17] Complications In the majority of instances, improvement ensues in the symptoms, while minor disability in the form of neck pain and headache persists in a small group of patients. Often, this occurs with the group that has a normal volume of posterior fossa while those with small PCF volumes show remarkable improvement. More than 85% are relieved of their head and neck pain. Nagib reported that minor forms of scoliosis, headache, neck pain and sleep apnea show good improvement [74] while those with syringomyelia and longstanding compression do not show satisfactory results. [17],[41] Nonspecific headache and sometimes aseptic meningitis may follow without or with dural repair. [61],[66] Conclusions CM constitutes an interesting clinical entity, where the embryological background still requires further studies. Recent imaging studies have increased the diagnostic ability of these anomalies enabling clinicians to adapt a conservative approach both in surgical and nonsurgical methods of management. [75] The spectrum of clinical presentation in children differs significantly from that of adults or adolescents. While early surgical correction is recommended for symptomatic cases, [76] incidental and asymptomatic malformations are best treated by watchful expectancy. References
Copyright 2010 - Neurology India The following images related to this document are available:Photo images[ni10003f2.jpg] [ni10003f5.jpg] [ni10003f6.jpg] [ni10003f3.jpg] [ni10003f4.jpg] [ni10003f1.jpg] [ni10003f7.jpg] [ni10003t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}