
|
Neurology India
Medknow Publications on behalf of the Neurological Society of India
ISSN: 0028-3886 EISSN: 1998-4022
Vol. 58, Num. 1, 2010, pp. 15-19
|
Neurology India, Vol. 58, No. 1, January-February, 2010, pp. 15-19
Review Article
Ophthalmoplegic migraine : Past, present and future
Vivek Lal
Department of Neurology, PGIMER, Chandigarh - 160 012, India
Correspondence Address: Dr. Vivek Lal, Department of Neurology,
PGIMER, Chandigarh – 160 012, India, vivekl44@yahoo.com
Date of Acceptance: 14-Feb-2010
Code Number: ni10004
DOI: 10.4103/0028-3886.60388
Abstract Ophthalmoplegic migraine (OM) is a rare disorder characterized by childhood onset, ophthalmoplegia and migraine headaches. The 3rd cranial nerve is commonly involved in recurrent attacks. Involvement of the sixth and fourth nerves is uncommon. GdMRI discloses enhancement of the nerves. Adult cases are rare and confined to case reports. A viral pathogenesis is considered to be the cause of OM in view of nerve enhancement. We look at the various aspects of OM in children and adults.
Keywords: Adults, children, migraine, ophthalmoplegia
Inroduction Ophthalmoplegic migraine (OM), is a unique disorder characterized by recurrent attacks of ophthalmoplegia, following severe migrainous headaches. [1],[2],[3] It was first recognized as such, by Charcot in 1890. [4] The condition almost always begins in childhood, and is considered to be rare in adults. [5],[6] However, OM may occur for the first time in adult life. [7],[8],[9],[10],[11],[12],[13],[14] The typical clinical picture of OM includes a child with severe migraine that lasts for several days and is followed soon after, by ptosis and diplopia due to isolated oculomotor nerve palsy, as the headache remits. Pupillary involvement with a ′full blown′ pupil is the rule in children. [3],[15],[16] However, pupillary sparing is not uncommon, especially in adults. [17],[18] Abducens nerve involvement is uncommon [2] and trochlear nerve palsy is rare. [9] Recovery is the rule. Rarely, deficits persist after multiple attacks. [2],[3] The incidence of OM is about 0.7 per million. [19] In a cohort of 5,000 patients with migraine, Friedman et al. found only eight patients with OM. [20] All the patients had childhood onset with multiple attacks of oculomotor nerve palsy. Lal et al. [18] reported 62 adult patients with OM in a cohort of 7,000 patients with migraine seen in a tertiary care hospital in India. These patients developed acute ophthalmoplegia with severe attacks of migraine. Isolated abducens palsy was seen in 35 (56.5%) patients at presentation thus suggesting that abducens nerve palsy is not as rare as previously reported. [7],[8],[10],[12] Ophthalmoplegic migraine: The past The criteria first proposed by Walsh and Hoyt [2] included: a) established history of typical migraine headaches, b) increasing severity of migraine (crescendo migraine) prior to the ophthalmoplegic attack, c) development of recurrent ophthalmoplegia with migraine pain, and d) exclusion of other causes of painful ophthalmoplegia with appropriate investigations, including a normal angiogram. These criteria were incorporated in the 1988 headache classification of the International Headache Society (IHS), and OM was included in the classification as a variant of migraine (1.3). [21] It was reasoned that during a severe migraine attack, the edematous wall of the ipsilateral carotid artery compresses the oculomotor nerve inside the cavernous sinus, besides narrowing the ostia of the vasa nervosa supplying the oculomotor nerve inside the cavernous sinus. [17],[22] Abnormal angiographic findings lent credence to this view. [22] Thus, depending on the presence or absence of pupillary involvement in patients with oculomotor palsy, a compressive [22] or ischemic etiology [17] was suspected. Ophthalmoplegic migraine: The present The advent of gadolinium magnetic resonance imaging (GdMRI) studies provided new insights into the pathogenesis of OM and triggered a sea change in the perception of the entity. The initial literature on MRI changes in OM was mostly confined to single case reports. Mark et al. [23] first described reversible enhancement of the third cranial nerve in OM. A year later, in 1993, Stommel et al. [24] reported an 18-year-old male with OM and recurrent right-sided pupil-involving third nerve palsy. GdMRI disclosed thickening and enhancement of the cisternal segment of the third nerve, that resolved on follow-up imaging five weeks later. Straube et al. [25] also reported similar enhancement of the third nerve in a single case of OM. In the first large series of OM in the post-MRI era in 1998, Mark et al. [26] reported six patients with recurrent third nerve palsy associated with thickening and enhancement of the involved nerves on GdMRI. These changes were evident in the cisternal segment of the third nerve and were most pronounced in the exit zone of the nerve from the midbrain. Follow-up GdMRI studies done after the resolution of ophthalmoplegia disclosed almost no enhancement. Based on their observations of the presence of reversible enhancement of the third nerve in OM, [23],[26] and its absence in ischemic diabetic cranial neuropathy, [23] Mark and colleagues [26] postulated a benign viral infection as the possible cause of OM. This view was subsequently endorsed by Lance and Zagami [16] who reported five patients of OM, including a patient with adult onset OM. One of their patients, a child, had recurrent attacks of OM following vaccination on three separate occasions. Based on these observations, and the presence of nerve edema and globoid appearance of the intracisternal part of the oculomotor nerve at the root exit zone the authors suggested that the syndrome might be caused by a recurrent demyelinating neuropathy, in which an inflammatory process affecting the oculomotor nerve might have irritated trigeminal sensory fibers present in the same nerve, triggering migraine headache. They felt that the pronounced thickening and enhancement of the third nerve, at its origin from the midbrain was due to intraneural edema, similar to that seen in inflammatory demyelinating neuropathies. In an accompanying editorial, Daroff [15] also endorsed this view and suggested shifting OM from `migraine′ to a `cranial neuralgia′ category. Carlow [3] also suggested a similar hypothesis of recurrent demyelination and remyelination leading to intraneural edema and enhancement of the third nerve, at its exit from the brainstem. A plethora of other case reports exhibiting similar findings on imaging, supported a post-viral demyelinating hypothesis. [27],[28],[29],[30],[31],[32] Based
on these incontrovertible GdMRI findings, OM was removed from the migraine
group and relegated to the neuralgia group. The revised IHS classification
proposed the following criteria for the diagnosis of OM:
a) At least two
attacks fulfilling criterion B.
b)
Migraine-like headache accompanied or
followed within four days of onset by paresis of one or more of the third,
fourth or sixth cranial nerves.
c)
Parasellar, orbital fissure, and posterior
fossa lesions ruled out by appropriate investigations.
Thus, the final exclusion of this jinxed entity [33] from a respectable position of being considered a migraine variant to being relegated to the cranial neuralgia group was solely based on the premise that because ischemic diabetic cranial neuropathy does not enhance, and OM enhances, it cannot be of ischemic origin. [26] Opthalmoplegic migraine was considered akin to post-viral and other demyelinating neuropathies. [15],[16] The severe migrainous headaches seen in almost all cases of OM were considered to be of secondary significance, without any relevance to its pathogenesis. Henceforth, OM was considered to be a post-viral demyelinating inflammatory neuropathy, without any relation to migraine or its pathogenic mechanisms. Besides cases with enhancement, lack of third nerve enhancement on GdMRI is also well documented in the literature. [9],[11],[18],[27],[28],[34],[35],[36] With the exception of a case report by Lee et al., [7] disclosing reversible enhancement of intraparenchymal abducens nerve on MRI, sixth nerve enhancement in OM has not been reported. [8],[10],[12],[13],[18]
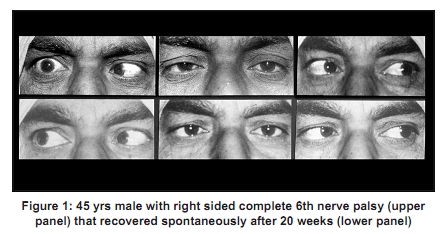
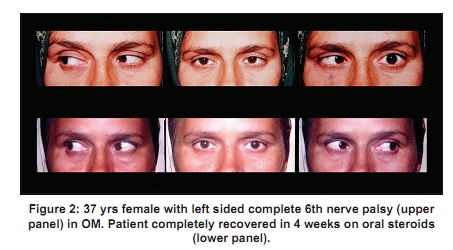
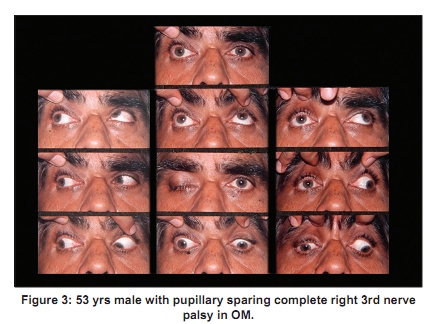
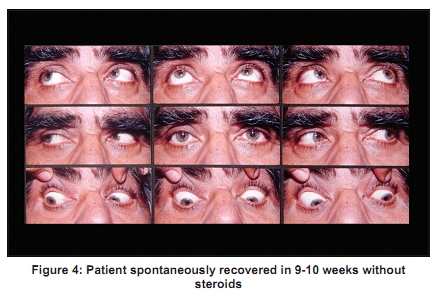
In a major break from traditional thinking, we reported 62 adult patients (age 15-68 years) of OM from India. [18] Almost all patients developed ophthalmoplegia during a severe migraine attack. An overwhelming majority of these patients had an antecedent worsening in severity of migraine headaches, before the ophthalmoplegic attack. Whereas 48 patients had a single attack, 14 patients had two or more attacks, fulfilling the IHS criteria for probable and definite OM, respectively. At presentation, isolated abducens, oculomotor and trochlear nerve involvements were seen in 35 (56%), 21 (33%) and five (8%) patients respectively. None of the patients had any nerve enhancement [Figure - 1],[Figure - 2],[Figure - 3],[Figure - 4],[Figure - 5]. Detailed cerebrospinal fluid (CSF) examination and biochemistry were normal. All patients recovered completely. Use of oral steroids hastened the recovery (P< 0.05). From India, Ravishankar and Kartik [36] also reported lack of enhancement in four patients of OM with involvement of third nerve. Borade et al. [37] recently reported a single pediatric case of OM, from Kerala, with enhancement of the third nerve. On the basis of our series, we suggest the following criteria for the diagnosis of a `pure′ case of OM.
a) History of established migraine before the first attack of OM. All
patients of OM developed against a backdrop of longstanding and uncontrolled
migraine.
b)
History of an antecedent worsening in severity of migraine before
the ophthalmoplegic attack. This important fact was also recognized by
Walsh and Hoyt. [2]
c)
Deficits develop during or within 24 h of a severe attack of migraine.
The ophthalmoplegic migraine attack is severe and often lasts beyond
24 h, even in children. [1],[21]
d)
No history of diabetes / hypertension / ischemic heart disease.
e)
No evidence
of vasculitis / active infection / malignancy / recent trauma.
f)
Normal
CSF examination. This has been a universal finding in all patients of
OM, even in patients with nerve enhancement.
g)
Positive family history of
migraine.
h)
GdMRI studies (1.5 Tesla Machine) should a) Disclose normal
cavernous sinuses on both sides, b) May show reversible nerve enhancement,
c) Not disclose any other pathology that may cause ophthalmoplegia.
i)
Conventional
angiogram / MR angio must be normal in all patients of OM.
j)
No evidence
of any other pathology on follow-up, that may cause ophthalmoplegia.
Ophthalmoplegic Migraine: The future As things stand today, OM is considered a recurrent inflammatory demyelinating illness of idiopathic or post-viral origin. [1],[5],[16] Migraine is considered secondary to irritation of fibers of the fifth nerve which accompany the inflamed third nerve. [15],[16] GdMRI imaging discloses reversible enhancement of the involved nerves. Resolution of ophthalmoplegia is the rule, with very few cases exhibiting permanent deficits often after recurrent attacks. [2],[3] Does a post-viral inflammatory hypothesis for OM account for other clinical features of OM? A hard look at the diagnostic criteria of OM is necessary before deciding the answer. Some of the issues include:
a) In spite of a postulated post-viral inflammation, a viral prodrome
is universally missing in cases of OM, both with and without enhancement. [2],[3],[7],[8],[9],[10],[11],[12],[13],[14],[15],[16],[17],[18],[19],[20],[21],[22],[23],[24],[25],[26],[27],[28]
b)
The CSF has consistently been normal in all patients of OM, both with
and without enhancement. [8],[9],[10],[11],[12],[16],[17],[18],[26],[27],[28] Indeed,
CSF was completely normal in four patients with OM reported by Mark et
al.[26] all
of whom had enhancement.
c)
Similarly, a post-viral hypothesis cannot account
for migraine associated with sixth and fourth nerve involvement.
d)
A post-viral
theory also cannot account for lack of enhancement of nerves.
Contrary to current thinking, migraine may have a definite role in the
pathogenesis of OM:
a) Literature testifies to the fact that almost all patients
of OM develop ophthalmoplegia with severe migraine, irrespective of age,
sex, presence or absence of nerve enhancement.
b)
All patients of OM have
a past history of typical migraine, which is similar to the ophthalmoplegic
attack.
c)
There is antecedent increase in severity of migraine headaches
prior to the onset of ophthalmoplegia.
d)
The migraine is invariably ipsilateral
to ophthalmoplegia.
e)
CSF is always normal.
For the above mentioned reasons, we feel that uncontrolled migraine may be the cause of OM. Activation of trigeminovascular system during an attack of migraine releases neuropeptides in the vessel wall. This causes a sterile inflammation of the wall of vasanervosa leading to a breach in the blood nerve barrier, which is formed by endothelium of vasanervosa. This leads to nerve edema and injury. Imaging may or may not show enhancement. There appears to be no difference in migraine headaches in patients with [3],[15],[27],[28] and without enhancement. [34],[38] Once the attack of OM subsides, the decrease in neurogenic inflammation of the vessel wall leads to restoration of the blood nerve barrier and decrease in nerve edema and enhancement. Thus, this hypothesis accounts for all facets of OM including antecedent severe migraine headaches and nerve enhancement. Recurrent attacks may result in nerve infarction and aberrant regeneration.
Are there subtypes of OM? It would be futile to divide OM into various subtypes as it is a heterogeneous disorder. However, based on our experience [18] and cases reported in world literature, [2],[3], [7],[8],[9],[10],[11],[12],[13],[14],[15],[16],[23],[24],[25],[26],[30],[31],[32],[33],[34],[35] we
would like to divide it into the following types:
a) Childhood variant:
This very well-described variant is characterized by onset in childhood,
severe migraine, recurrent third nerve palsy with pupillary involvement,
and enhancement on GdMRI. Rarely, it is painless [2] and
lacks enhancement. [2],[27],[28],[36]
b)
The adult variant: It is characterized by adult onset, severe migraine,
an antecedent worsening in severity of migraine prior to the ophthalmoplegic
attack, and single attacks of sixth nerve palsy. [18] Third
nerve involvement is less common and it is pupillary-sparing. Enhancement
is uncommon even with third nerve involvement. [5],[9],[11],[34],[35],[36]
Conclusions
No complication of migraine has generated so much discussion as OM. Yet, there appears to be no consensus on this issue. Recent publications are eloquent of this discord. [5],[18],[35],[36],[39] In our opinion, reducing migraine to a secondary spectator in the pathogenesis of OM, would be turning a Nelson′s eye to the obvious. Its uniform and overwhelmingly severe presence in all cases of OM, irrespective of the type of cranial nerve involvement, cannot be ignored. Socrates said, "I cannot make people learn, I can only make them think". We hope to have succeeded in doing that.
References
| 1. | Headache Classification Subcommittee of the International Headache Society. The international classification of headache disorders. Cephalalgia 2004;24:1-160. Back to cited text no. 1 |
| 2. | Walsh FB, Hoyt NF. Clinical neuro-ophthalmology. Baltimore, MD: Williams and Wilkins; 1969. Back to cited text no. 2 |
| 3. | Carlow TJ. Oculomotor ophthalmoplegic migraine: is it really migraine. J Neuroophthalmol 2002;22:215-21. Back to cited text no. 3 [PUBMED] |
| 4. | Charcot JM. Sur un cas de migraine ophthalmoplegique (paralysie oculo-motrice periodique). Progr Med (Paris) 1890;31:83-6; 32:99-102. Back to cited text no. 4 |
| 5. | Ravishankar K. Ophthalmoplegic migraine: still a diagnostic dilemma? Curr Pain Headache Rep 2008;12:285-91. Back to cited text no. 5 [PUBMED] |
| 6. | Levin M, Ward TN. Ophthalmoplegic migraine. Curr Pain Headache Rep 2004;8:306-9. Back to cited text no. 6 [PUBMED] |
| 7. | Lee TG, Choi WS, Chung KC. Ophthalmoplegic migraine with reversible enhancement of intra-parenchymal abducens nerve on MRI. Headache 2002;42:140-1. Back to cited text no. 7 [PUBMED] |
| 8. | Verhagen WIM, Prick MJJ, Azn Dijk van R. Onset of ophthalmoplegic migraine with abducens palsy at middle age? Headache 2003;43:798-800. Back to cited text no. 8 |
| 9. | van der Dussen DH, Bloem BR, Liauw L, Ferrari MD. Ophthalmoplegic migraine: Migrainous or inflammatory? Cephalalgia 2004;24:312-5. Back to cited text no. 9 |
| 10. | Celebisoy N, Sirin H, Gokcay F. Ophthalmoplegic migraine: two patients, one at middle age with abducens palsy. Cephalalgia 2004;25:151-3. Back to cited text no. 10 |
| 11. | Sullivan SS, Regan KN, Tormey P, Galvin RJ. Late-onset ophthalmoplegic migraine in a patient with previous childhood abdominal migraine. Cephalalgia 2006;26:1022-35. Back to cited text no. 11 |
| 12. | Crevits L, Verschelde H, Casselman J. Ophthalmoplegic migraine: an unresolved problem. Cephalalgia 2006;26:1255-9. Back to cited text no. 12 [PUBMED] |
| 13. | Mucchiut M, Valentinis L, Provenzano A, Cutuli D, Bergonzi P. Adult-onset ophthalmoplegic migraine with recurrent sixth nerve palsy: a case report. Headache 2006;46:1589-1. Back to cited text no. 13 [PUBMED] |
| 14. | Mark AS, Blake P, Atlas SW, Ross M, Brown D. Enhancement of the cisternal portion of the third nerve on gadolinium - enhanced MR images: Clinical and Pathologic correlation (abstract). Radiological Society of North America 77th Scientific Assembly and Annual Meeting, Vol 28. 1991. Back to cited text no. 14 |
| 15. | Daroff RB. Ophthalmoplegic migraine. Cephalalgia 2001;21:81. Back to cited text no. 15 [PUBMED] |
| 16. | Lance JW, Zagami AS. Ophthalmoplegic migraine: A recurrent demyelinating neuropathy? Cephalalgia 2001;21:84-9. Back to cited text no. 16 [PUBMED] |
| 17. | Vijayan N. Ophthalmoplegic migraine: ischemic or compressive neuropathy? Headache 1980;20:300-4. Back to cited text no. 17 [PUBMED] |
| 18. | Lal V, Sahota P, Singh P, Gupta A, Prabhakar S. Ophthalmoplegia with migraine in adults: Is it ophthalmoplegic migraine? Headache 2009;49:838-50. Back to cited text no. 18 [PUBMED] |
| 19. | Hansen SL, Borelli-Moller L, Strange P, Nielsen BM, Olesen J. Ophthalmoplegic migraine: Diagnostic criteria, incidence of hospitalization and possible etiology. Acta Neurol Scand 1990;81:54-60. Back to cited text no. 19 |
| 20. | Friedman AP, Harter DH, Merritt HH. Ophthalmoplegic migraine. Arch Neurol 1962;7:320-7. Back to cited text no. 20 [PUBMED] |
| 21. | Headache Classification Committee of the International Headache Society: Classification and diagnostic criteria for headache disorders, cranial neuralgias and facial pain. Cephalalgia 1988;8:1-96. Back to cited text no. 21 |
| 22. | Walsh JP, O'Doherty DS. A possible explanation of the mechanism of ophthalmoplegic migraine. Neurology 1960;10:1079-84. Back to cited text no. 22 [PUBMED] |
| 23. | Mark AS, Blake P, Atlas SW, Ross M, Brown D, Kolsky M. Gd-DTPA enhancement of the cisternal portion of the oculomotor nerve on MR imaging. AJNR Am J Neuroradiol 1992;13:1463-70. Back to cited text no. 23 [PUBMED] |
| 24. | Stommel EW, Ward TN, Harris RD. MRI findings in a case of OM. Headache 1993;33:93-4. Back to cited text no. 24 |
| 25. | Straube A, Bandmann O, Büttner U, Schmidt H. A contrast enhanced lesion of the III nerve on MR of a patient with ophthalmoplegic migraine as evidence for a Tolosa-Hunt syndrome. Headache 1993;33:446-8. Back to cited text no. 25 |
| 26. | Mark AS, Casselman J, Brown D, Sanchez J, Kolsky M, Larsen TC 3rd, et al. Ophthalmoplegic migraine: reversible enhancement and thickening of the cisternal segment of the oculomotor nerve on contrast-enhanced MR images. Am J Neuroradiol 1998;19:1887-91. Back to cited text no. 26 [PUBMED] |
| 27. | Prats JM, Mateos B, Garaizar C. Resolution of MRI abnormalities of the oculomotor nerve in childhood ophthalmoplegic migraine. Cephalalgia 1999;19:655-9. Back to cited text no. 27 [PUBMED] |
| 28. | Ostergaard JR, Moller HU, Christensen T. Recurrent ophthalmoplegia in childhood: diagnostic and etiologic considerations. Cephalalgia 1996;16:276-9. Back to cited text no. 28 |
| 29. | Wong V, Wong WC. Enhancement of oculomotor nerve: a diagnostic criterion for ophthalmoplegic migraine? Pediatr Neurol 1997;17:70-3. Back to cited text no. 29 [PUBMED] |
| 30. | Aers I, Van Zandijcke M, Dehaene I. Magnetic resonance imaging in a case of migraine with ophthalmoplegia. Eur J Neurol 1997;4:85-9. Back to cited text no. 30 |
| 31. | O'Hara MA, Anderson RT, Brown D. Magnetic resonance imaging in ophthalmoplegic migraine of children. J AAPOS 2001;5:307-10. Back to cited text no. 31 |
| 32. | Ramelli GP, Vella S, Lövblad K, Remonda L, Vassella F. Swelling of the third nerve in a child with transient oculomotor paresis: a possible cause of ophthalmoplegia migraine. Neuropediatrics 2000;31:145-7. Back to cited text no. 32 |
| 33. | Daroff RB. Random comments: neurologists and neuro-ophthalmology: the ocular motor system: update on ophthalmoplegic migraine. Sem Neurol 2000;20:145-9. Back to cited text no. 33 |
| 34. | De Silva DA, Siow HC. A case report of ophthalmoplegic migraine: a differential diagnosis of third nerve palsy. Cephalalgia 2005;25:827-30. Back to cited text no. 34 [PUBMED] |
| 35. | Lane R, Davies P. Ophthalmoplegic migraine: The case for reclassification. Cephalalgia 2009;29:1-8. Back to cited text no. 35 |
| 36. | Ravishankar K, Karthik G. Ophthalmoplegic migraine - suggestions for revision of nosology based on normal imaging in four patients (abstract). Cephalalgia 2007;27:1182. Back to cited text no. 36 |
| 37. | Borade A, Prabhu AS, Kumar S, Prasad V, Rajam L. Magnetic resonance imaging findings in ophthalmoplegic migraine. J Postgrad Med 2009;55:137-8. Back to cited text no. 37 [PUBMED]  |
| 38. | Shin DJ, Kin JH, Kang SS. Ophthalmoplegic migraine with reversible thalamic ischemia shown by brain SPECT. Headache 2002;42:132-5. Back to cited text no. 38 |
| 39. | Friedman DI. The ophthalmoplegic migraines: A proposed classification. Cephalalgia 2009;29:1-2. Back to cited text no. 39 |
Copyright 2010 - Neurology India
The following images related to this document are available:
Photo images
[ni10004f5.jpg]
[ni10004f3.jpg]
[ni10004f2.jpg]
[ni10004f4.jpg]
[ni10004f1.jpg]
|

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}