 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 58, No. 1, January-February, 2010, pp. 24-28 Original Article Anatomical variations of the sural nerve in the leg: A fetal study Nachiket Shankar, Robert Patrick Selvam, Nikhil Dhanpal, Ravikanth Reddy, Ashok Alapati Department of Anatomy, St. John’s Medical College, Bangalore, India Correspondence Address: Dr. Nachiket Shankar, Department of Anatomy, St. John’s Medical College, Sarjapur Road, Bangalore - 560 034, Karnataka, India, nachiket76@gmail.com Date of Acceptance: 18-Aug-2009
Code Number: ni10006 DOI: 10.4103/0028-3886.60390 Abstract Background : Because of its clinical importance, numerous studies
have been conducted worldwide documenting the anatomical variations of
the sural nerve (SN). However, there is a paucity of literature from
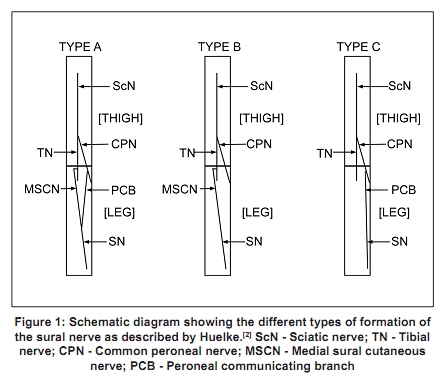
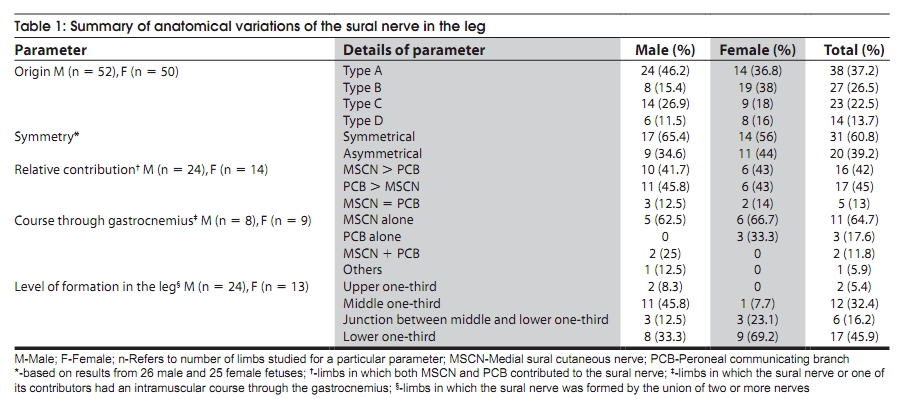
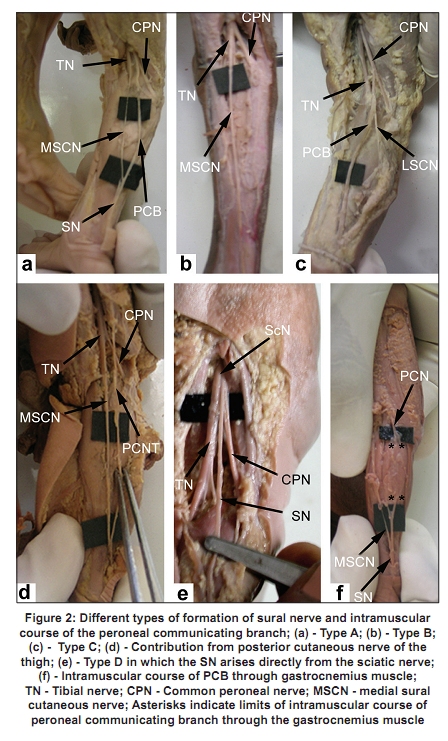
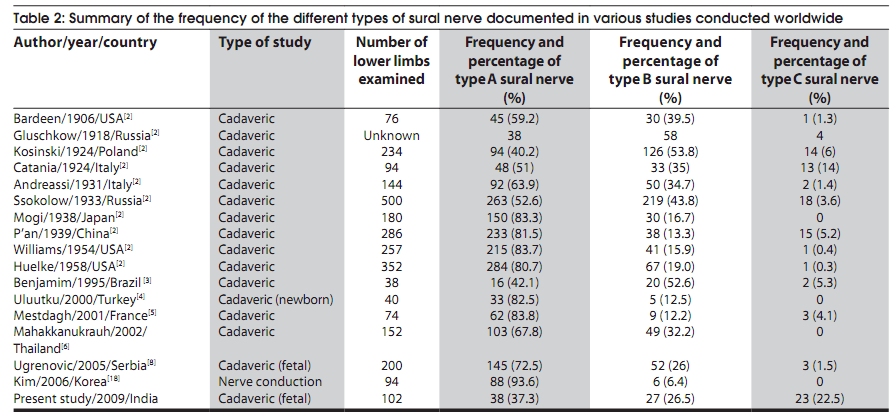
India concerning the anatomical variations of the SN in the leg. Keywords: Anatomical variations, fetuses, leg, sural nerve Introduction The sural nerve (SN) is clinically important, as it is commonly used for nerve conduction studies, nerve biopsies, and as a convenient source for nerve grafting. [1] It is usually described as being formed by the direct continuation of the medial sural cutaneous nerve (MSCN), a branch of the tibial nerve (TN), or as the union between the MSCN and the peroneal communicating branch (PCB) of the common peroneal nerve (CPN). [2] Numerous studies have been conducted worldwide documenting the anatomical variations of the SN. [2],[3],[4],[5],[6],[7],[8],[9] Studies conducted in India have described the pattern of cutaneous distribution of the SN in the foot, the variability of sensory deficit following SN biopsy, as well as the results of surgeries utilizing flaps containing the SN. [10],[11],[12],[13] However, there is a paucity of literature from India concerning the anatomical variations of the SN in the leg. The present study documents the anatomical variations of the SN in the leg in Indian fetuses, and discusses the findings. Materials and Methods One hundred and two lower limbs from 51 embalmed fetuses of Indian origin (26 male and 25 female) were studied. All the fetuses were available at the Department of Anatomy in the medical college to which the authors are attached. The crown-rump (CR) length of the fetuses ranged from 13 cm to 41 cm (mean - 27.7 cm; standard deviation ± 5.4 cm). The dissection of the lower limbs was conducted as follows. A longitudinal skin incision was made from the gluteal fold, till the prominence of the heel along the midline of the limb as described by Ugrenovic et al. [8] Horizontal incisions were made at the ends of this incision and the skin flaps were reflected. The SN was identified in the lower one-third of the leg where it became superficial. It was then traced upwards through the deep fascia till its origin, and distally to the level of the lateral malleolus. All contributions to the SN were noted and their diameters measured using digital Vernier calipers. The origin of the SN was classified into Type A, B and C as described by Huelke [Figure - 1]. [2] Type A was the anastomotic type, in which both the MSCN and the PCB contributed to the formation of the SN. When the SN was formed only by the MSCN it was designated as Type B, while if it was formed by the PCB alone it was classified as Type C. The presence or absence of bilateral symmetry with respect to the type of SN was noted. When Type A SN was observed, the relative contributions of the MSCN and the PCB were documented. Any intramuscular course of the above nerves through the gastrocnemius muscle was noted. If the SN was observed to be formed by more than one contribution, the level of union was noted with respect to the upper, middle or lower third of the leg. After calculating relevant percentages, the findings were tabulated. Results The results of the study are summarized in [Table - 1]. The origin of the SN was highly variable. When male and female fetuses were considered together, the SN was most commonly of Type A (38 limbs of 102, 37.2%) [Figure - 2]a. This mode of origin of the SN was the most common one in males [Table - 1]. In eight (eight of 38, 21.1%) of these limbs the MSCN and the PCB did not unite and coursed separately. Two (two of 38, 5.3%) and one limb (one of 38, 2.6%) showed an origin of the PCB and the MSCN from the sciatic nerve (ScN) respectively. The posterior cutaneous nerve of the thigh (PCNT) was associated with three of the 38 limbs (7.9%) in which Type A SN was observed. Less common origins of the SN were Type B (27 limbs of 102, 26.5%) [Figure - 2]b and Type C (23 limbs of 102, 22.5%) [Figure - 2]c. Type B was the most common one in females [Table - 1]. The PCNT was associated in two limbs each with Type B (two of 27, 7.4%) and Type C (two of 23, 8.7%) [Figure - 2]d. In 14 (14 of 102, 13.7%) limbs the SN arose directly from the ScN alone, close to its division into its terminal branches, the TN and the CPN [Figure - 2]e. This mode of origin of the SN was designated as Type D. Multiple roots (usually two, rarely three) of the MSCN and PCB contributing to the formation of the SN were observed in seven (seven of 102, 6.9%) limbs. Of these, in five (five of seven, 71.4%) of the limbs the PCB showed multiple roots, while in two (two of seven, 28.6%) of the limbs the MSCN was similarly formed. The MSCN and the PCB were observed in 65 (65 of 102, 63.7%) and 61 (61 of 102, 59.8%) limbs respectively. The PCB was observed as a branch of the lateral sural cutaneous nerve (LSCN) in nine (nine of 61, 14.8%) of the limbs [Figure - 2]d. The mode of origin of the SN was considered symmetrical if it was similar bilaterally. Bilateral symmetry of origin was noted in 31 of the 51 fetuses (60.8%) [Table - 1]. Of these, in 13 (13 of 51, 41.9%) fetuses, the SN was of Type A. In eight (eight of 51, 25.8%) and six (six of 51, 19.4%) fetuses respectively, the SN was of Type B and C. Four (12.9%) fetuses of Type D showed a symmetrical origin of the SN. The frequency of bilateral symmetry within a particular of type of SN differed. Bilateral symmetry of Type A SN was noted in 26 of 38 (68.4%) limbs. In 16 of 27 (59.3%) limbs of Type B SN and 12 of 23 (52.2%) of Type C SN bilateral symmetry was observed. Of the 38 limbs in which Type A SN was observed, the MSCN was found to be larger in 16 limbs (42.1%) and the PCB was found to be larger in 17 limbs (44.7%). In five limbs (13.2%) the relative contribution of the MSCN and PCB was equal [Table - 1]. The formation of the SN by the union of two or more nerves was noted in 38 limbs. The site of union was noted in the lower two-thirds of the leg in 36 limbs (95%). In only two limbs (5%) was the site of union observed in the upper one-third of the leg [Table - 1]. However, differences were noted among the sexes. In males the commonest site of union was the middle one-thirds, while in females it was the lower one-thirds of the leg. An intramuscular course of the SN or one of its contributors through the gastrocnemius was seen in 17 limbs (17 of 102 limbs, 16.7%) [Figure - 2]f. In four fetuses (8 of 17 limbs, 47.1%) this was observed bilaterally. Of the 17 limbs, an intramuscular course of the MSCN was observed in 11 limbs (64.7%). Less commonly noted was an intramuscular course of the SN or its other contributors [Table - 1]. The other variation observed was a high division of the ScN in 11 limbs (10 of 102, 9.8%), more commonly in females (seven of 50 limbs, 14%) than in males (three of 52 limbs, 5.8%). Of the female limbs, five of seven (71.4%) showed Type BSN, and one each, Type C (14.3%) and Type D (14.3%) SN. In males, in two of three limbs (66.7%) Type A SN was noted and in one limb (33.3%) Type D SN was noted. Discussion P′an was the first investigator to classify the SN into three types (A,B and C) based on its origin. [2],[14] The term sural nerve complex (SNC) was first used by Ortiguela et al., to refer to the MSCN, LSCN, PCB and SN. [8],[15] Subsequently, some authors have proposed more detailed methods of classifying the origin of the SN based on the SNC. [3],[4],[5],[8] With respect to the origin of the SN, the results of the above mentioned studies, including those of the present study are summarized in [Table - 2]. The major difference in the present study as compared to previous studies is the higher incidence (22.5%) of Type C and a lower incidence (37.3%) of Type A SN. Also, the origin of the SN as a single branch from the ScN near its termination has not been described. In the present study this was seen in 14 (13.7%) limbs and was designated as Type D. Previous studies did not show any correlation between sex and type of SN. [4],[8] However, in the present study Type A was more common in males and Type B in females. The incidence of Type A SN in which the MSCN and PCB do not unite (7.8%) was similar to the results of Mestdagh et al. [5] Other authors have reported a slightly lower frequency of 5% and 6.77%. [8],[16] The origin of the MSCN or PCB from the ScN were observed with a similar frequency to previous studies. [8] The use of the SN as a nerve graft or for peripheral nerve biopsy is often associated with chronic pain and persistent sensory loss. [17] This has led to the suggestion to utilize the MSCN or PCB as a substitute for the SN in the above procedures to reduce complications. [18] However, if Type B, C, or D SN is present, as the majority of the SN in the present study, this would not be advantageous. Also, the great variability in the origin of the SN needs to be considered when the sural sensory nerve action potential is of low amplitude and disproportionate to the neurologic evaluation. [9] The incidence of the PCNT in the vicinity of the SN in the present study (6.9%) was slightly higher as compared to earlier studies which showed a frequency of 5% and 4.5%. [4],[8] Multiple roots of either the PCB or MSCN were more often observed (6.9%) in the present study than those reported previously (2.5% and 0.5%). [4],[8] In previous studies, the PCB was seen to be formed by multiple roots, but not the MSCN. [4],[8] A survey of the literature showed great variations in the origin of the PCB. Some investigators report that the PCB is more often a branch of the LSCN [5],[8],[15] while others report that it is commonly a branch of the CPN. [4],[16] The present study concurs with the latter observation. In the authors′ opinion, the classification proposed by P′an is simple but comprehensive. Any variations can be classified as subtypes based on, the origin of the MSCN and the PCB, contributions if any from the PCNT, the presence of multiple roots and whether or not the nerves contributing to the SN unite. The MSCN can arise from the TN or more rarely from the ScN. The PCB on the other hand may arise from the CPN, LSCN or the ScN. The PCNT could contribute to any of the types. Also, multiple roots of any of the contributors to the SN may be present. When multiple nerves contribute to the formation of the SN, these may or may not unite. The origin of the SN from the ScN alone may be classified as Type D. The explanation for finding a greater frequency of origin of the SN or one of its contributors from the ScN may be related to age, race, and method of dissection. Uluutku et al., have suggested that there may positional changes in nerves during life. [4] Ugrenovic et al., have stated that in their study, an incision was made from the gluteal region to the heel, thus contributing to full exposure of the ScN and its branches. [8] A similar method of exposure was followed in the present study. The frequency of bilateral symmetry in the origin of the SN observed in this study (60.8%) was lower as compared to other studies conducted, which showed an incidence ranging from 62% to 83.9%. [2],[4],[8] The frequency of bilateral symmetry within particular types, was similar to other studies, [2],[8] except for Type C, which showed a much higher incidence of bilateral symmetry in the present study. This could be related to the greater frequency of Type C in this study. The relative contribution of the MSCN and PCB to Type A SN has been studied in cadavers as well as by nerve conduction studies. [4],[6],[15],[18],[19],[20] Some of these studies have shown a greater contribution from the MSCN [4],[18],[19],[20] while others authors have reported a more substantial contribution from the PCB. [6],[15] In the present study, the relative dominance of the PCB contribution as compared to the MSCN was observed slightly more frequently. Some investigators have observed that Type A SN is frequently formed in the middle one-third of the leg. [4],[5],[8],[16] Others have reported that it is more commonly formed in the lower one-third of the leg. [6],[9],[21],[22] None of the authors have reported any sexual differences in the site of formation of the SN. In the present study, when the SN was formed by the union of two or more nerves (either Type A or multiple roots of other types), the lower one-third of the leg was found to be the most common site of formation of the SN. However, the middle one-third of the leg was the commonest site of formation of the SN in males, while it was the lower one-third in females. An intramuscular course of the MSCN through the gastrocnemius was noted in 6.7% of 60 legs in a study conducted in Brazil. In one cadaver this was found bilaterally. [23] A recent case report also describes this finding unilaterally. [24] Only one case report of the SN arising entirely from the PCB and also having an intramuscular course through the gastrocnemius muscle has been described so far. [25] An intramuscular course of the SN or one of its contributors was found more frequently in the present study (16.7%). This was bilaterally observed in 47.1% of these limbs. Most commonly, the MSCN had an intramuscular course. Rarely, the PCB as well as the SN, if it was formed in the upper half of the leg, were also observed to take such an intramuscular course [Table - 1]. Many studies have documented symptoms produced by the entrapment of the SN by fascia or scar tissue. However, penetration of the gastrocnemius by the SN has been rarely described. This anomalous course should be considered in any pain that occurs in the distribution of the SN due to suspected entrapment. [23] In a study conducted on 200 fetal lower limbs in Serbia a high division of the ScN was noted in 27.5% of the limbs. [26] A study conducted in Poland on 36 adult lower limbs also showed a similar incidence of high division of the ScN. [27] In the present study the frequency of high division of the ScN was lower (9.8%). This was most commonly seen in females, and associated with Type B SN, the other types being less frequently observed. The high division of the ScN has to be kept in mind while performing popliteal block anesthesia. [26] The limitations of the present study are mentioned below. As this study was done on fetuses, small contributions to the SN might have been inadvertently damaged or overlooked. In addition, due to changes in caliber and position of nerves with age, it is not certain whether these results are applicable to Indian adults. Also, some of these fetuses may have suffered from congenital malformations or genetic abnormalities which were incompatible with life. The role of a possible association of a particular type of SN with a particular congenital malformation or genetic abnormality cannot be ruled out. Acknowledgments The authors would like to thank Dr. Roopa R and Dr. V Balasubramanyam, Professors, Department of Anatomy, St. John′s Medical College, Bangalore for their support and encouragement. We are also grateful to the attenders working in the anatomy department for helping us out during the dissections. References
Copyright 2010 - Neurology India The following images related to this document are available:Photo images[ni10006f1.jpg] [ni10006t2.jpg] [ni10006t1.jpg] [ni10006f2.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}
{kind=link}