 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 58, No. 1, January-February, 2010, pp. 42-47 Original Article Quantitative videofluoroscopic analysis of penetration-aspiration in post-stroke patients Li Bingjie, Zhang Tong, Sun Xinting, Xu Jianmin1 , Jiang Guijun1 Departments of Neurorehabilitation, 1 Radiology, Capital Medical University School of Rehabilitation Medicine, Rehabilitation Research Center, No.10 JiaoMenBei Lu, Beijing - 100 068, China Correspondence Address: Dr. Zhang Tong, Department of Neurorehabilitation, Capital Medical University School of Rehabilitation Medicine, China Rehabilitation Research Center, No.10 JiaoMenBei Lu, Beijing - 100 068, China, kaka0515@sohu.com Date of Acceptance: 02-Jul-2009
Code Number: ni10009 DOI: 10.4103/0028-3886.60395 Abstract Background : Dysphagia is a common complication of stroke and
is a potential cause for aspiration and malnutrition and is also associated
with poor outcome. Videofluoroscopic Swallowing Study (VFSS) is the most
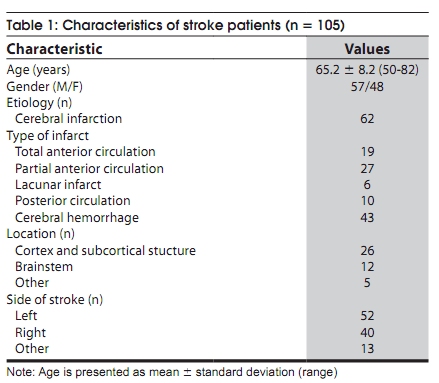
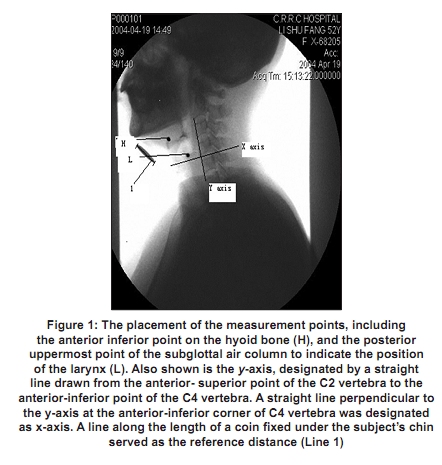
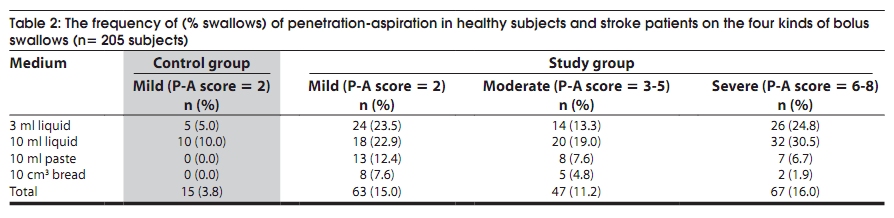
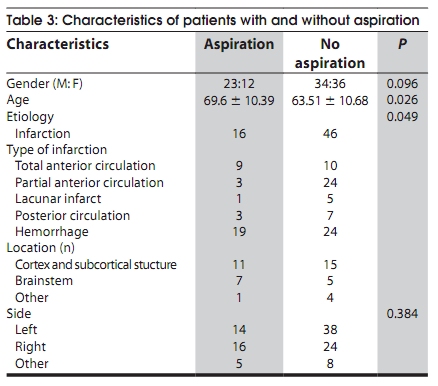
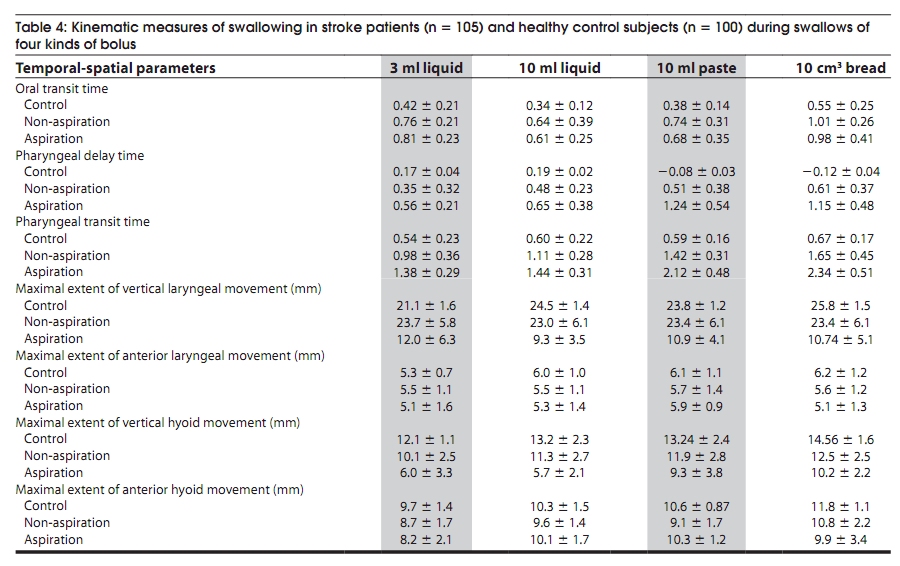
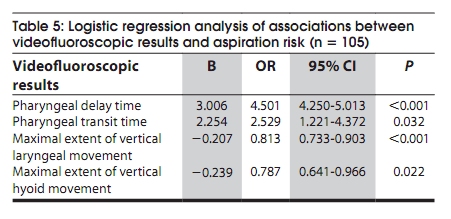
objective method for evaluation of swallowing disorders. Keywords: Stroket, dysphagi, kinematic analysis, penetration-aspiration, videofluoroscopic swallowing study Introduction Dysphagia is a common complication of stroke and swallowing difficulties with penetration-aspiration can affect 22% to 70% stroke patients, depending on the timing of the study, methodology, and diagnostic criteria. [1],[2],[3] The swallowing difficulty may persist in some patients for many months. [4],[5],[6] Accidental dropping of food or liquids into the airway while eating or drinking is perhaps the most common consequence of dysphagia in clinical practice Airway invasion may be described as penetration, foreign material not passing below the vocal folds and aspiration, foreign material passing below the vocal folds into the trachea, possibly beyond. Accurate and efficient evaluation of the swallowing abnormalities in patients with dysphagia is critical for an appropriate and effective treatment. Videofluoroscopic Swallowing Study (VFSS) is a well-established objective method for the real-time evaluation of the swallowing process. The significant advantage of the VFSS is that it provides objective assessment of penetration-aspiration and also frequently identifies the underlying cause(s) for penetration-aspiration. Previous videofluoroscopic studies were focused on description of the severity of penetration-dysphagia qualitatively. In most of these studies, the presence or absence of penetration-aspiration was used to determine swallowing function. [4],[5],[7] However, this binary forced-choice method may not accurately reflect the variability in airway invasion. The Penetration-Aspiration Scale (P-AS) is an ordinal scale that evaluates airway invasion with more accurate and reliable determination of severity. [8] Contemporary clinical observations of videofluoroscopic examination of the oropharyngeal swallowing function have suggested that invasion of food or liquids into the vocal folds is often associated with other risk factors of oropharyngeal dysphagia such as alterations of swallowing movement and bolus flow. Thus it is imperative to recognize the risk factors associated with aspiration before developing management strategies for dysphagia. Subtle swallowing abnormalities can be identified with quantitative measures by VFSS. Several studies in the recent years have identified a range of penetration-aspiration and kinematic characteristics of swallow. [9],[10],[11] However, the characteristics distinguishing stroke patients from healthy subjects, and the relationship between penetration-aspiration and kinematic parameters have not been fully investigated. The aim of this study was to describe the occurrence and characteristics of penetration-aspiration in post-stroke patients and healthy control subjects using P-AS and also to determine the relationship between aspiration and kinematic parameters of swallow. Materials and Methods Subjects A total of 105 consecutive stroke patients admitted in our center between April 2004 and May 2007 were included in the study. All the patients were consciousness (Glasgow Coma Scale> 10) and medically stable, with no previous history of swallowing impairment or a medical condition that could affect swallowing function. All patients were assessed neurologically to establish the diagnosis of stroke and the pathological and etiological subtype of stroke. Patients who were unable to maintain a sitting posture or whose cognitive functions were too poor to follow the instructions were excluded from the study. There were 57 men and 48 women, with the age ranging from 50 to 82 years (mean = 65.2 ± 8.2 years). The time for initial videofluoroscopy was 43 ± 20 days (range, 11-85 days) from the onset. Thirty-eight patients had no history of stroke. The diagnosis of ischemic stroke sub-type was based on the Oxfordshire classification. [12] The baseline data of the patients are provided in [Table - 1]. Control subjects were 100 medically healthy males (mean age ± standard deviation [SD] = 62 ± 9 years, range 50-78 years), None of the patients had any coexisting neurological diseases that can account for dysphagia. Average age was comparable among the three groups (χ2 test, χ2 = 0.51; P = 0.684). All study protocols were presented to and approved by our Hospital Ethical Committee, and all participants signed written consent before recruitment. Videofluoroscopic study of swallowing Standardized VFSS was conducted with a digital fluoroscope (Diagnost 76 Plus; Philips, Eindhoven, the Netherlands) which could provide real-time dynamic and frame-by-frame static images. A graphic time display provided by an RCA (Indianapolis, IN) character generator and JVC (Wayne, NJ) alternating-current adapter (Model C412) was included on the videotape so that information of timing at 0.01 second intervals was recorded. The swallowing studies were recorded with 30 frames per sec. The software program for spatial analysis of dicom images was a free DICOM viewer program Xiphoid 1.3 (developed by Ning Ging, MS. Huaxi Medical University, China). Spatial measurements were made after calibration of the digitized image with a 2.5 cm diameter radio-opaque coin taped to the chin at midline of the subject. Participants were instructed to sit upright and observed laterally. The fluoroscopic tube was focused on the lips anteriorly, the cervical veterbrae posteriorly, the soft palate superiorly, and bifurcation of the airway and esophagus inferiorly. Each participant swallowed in sequence, four standardized formulas, including 1 ml and 10 ml of thin liquid barium, 10 ml applesauce mixed barium, and 10 cm 3 biscuit coated with barium. A videofluoroscopic evaluation outlined by Logemann [13] was conducted in 205 subjects in the two groups. The total screening time was controlled below 80 secs for all the patients, so as to ensure a radiation dose of < 0.3 m Sv. Results of the evaluations were reviewed by at least two observers, before a swallowing diagnosis was formulated. Airway invasion was determined using P-AS [14] The scores of this scale range from 1 to 8. Score 1 indicates no penetration-aspir ation, which means no bolus enters airway. Score 2 indicates that bolus enters the airway but remains above vocal folds with clearing, and the classification is mild. Scores 3 to 5 indicate that bolus enters the airway without clearing or adheres to vocal cords but does not pass through the vocal folds, and the classification is moderate. Scores 6 to 8 indicate that bolus passes through the vocal folds into the trachea, and the classification is severe. In this study, the points, lines, and angles were marked on each digitized video frame as is illustrated in [Figure - 1]. A reference coin was stuck to the chin of the patients to allow the quantification in different dimensions. A straight line drawn from the anterior-superior point of the C2 vertebra to the anterior-inferior point of the C4 vertebra was designated as y-axis. The x-axis (x) was a straight line perpendicular to the y-axis. A point on the anterior-inferior corner of C4 vertebra was used as the zero point. Point H on the most anterior-superior aspect of the hyoid bone represents hyoid movement. Point L on the posterior-superior corner of the subglottic air column represents laryngeal movement; Line 1 represents a line along the length of a radio-opaque coin fixed under the subject′s chin to serve as the reference ruler to compensate the radiographic magnification. An experienced doctor observed the temporal measures of the bolus movement during the swallowing and maximal extent of structural movement: (1) oral transit time (OTT): From the initiation of posterior bolus movement to arrival of the bolus head at ramus of the mandible; (2) pharyngeal delay time (PDT): From the time bolus head passing ramus of the mandible to the beginning of laryngeal elevation; (3) pharyngeal transit time (PTT): From the arrival of bolus head at ramus to the time bolus tail passing through upper esophageal sphincter. Maximal extent of structural movement (in mm) includes: (4) vertical laryngeal movement; (5) anterior laryngeal movement; (6) vertical hyoid movement; (7) anterior hyoid movement. All measures of structural movement were showed with the videoframe which provides the images of the whole process of swallowing. Statistical analysis All analyses were performed with the SPSS 14.0 System statistical software and P < 0.05 was considered significant and P < 0.001 was considered highly significant. The c2 test was used to compare the P-AS scores of four boluses′ swallowing between two groups. Student′s t test or the c2 test was utilized to compare the characteristics of patients with and without aspiration. All kinematic data reported in the results were presented as mean ± SEM. Description and comparison of performance between subjects was made by analysis of variance (ANOVA).The association of kinematic parameters and penetration-aspiration was analyzed with logistic regression model. As the kinematic parameters were independent variables, we calculated the odds ratio (OR). We also calculated the 95% confidence interval (CI) and its respective P value by means of a logistic regression analysis model. Results The occurrence of penetration-aspiration The data concerning penetration-aspiration are given in [Table - 2]. One hundred normal subjects did 400 swallows and none of them had moderate or severe penetration-aspiration (score 3-8). Five (5%) normal subjects scored a score of 2 while swallowing 3 ml liquid bolus and 10 (10%) normal subjects scored a score of 2 while swallowing 10 ml liquid bolus. One hundred and five post-stroke patients performed a total of 420 swallows. There were mild penetrations (score 2) in 63 (15%); moderate penetrations (score 3-5) in 47 (11.2%) and 35 (33.3%) patients experienced one or more aspirations during examination. Aspirations (score 6-8) were presented in 67 (16%) patients. The stroke group scored significantly higher scores on the P-AS than did the control group (χ2 test, P < 0.001). Characteristics of 35 aspirators are shown in [Table - 3]. The gender difference between patients with and without aspiration was not significantly different. Aspiration was more frequent in elder patients ( P = 0.026) or patients with hemorrhagic stroke ( P = 0.049). The differences in the subtype of infarction and the location of hemorrhage between aspirators and non-aspirators could not be identified because of insufficient samples. Kinematic measures of swallowing Kinematic measures of swallow in stroke patients ( n = 105) and healthy control subjects ( n = 100) during swallows of four types of boluses are shown in [Table - 4]. Aspirating patients had delayed PDT and prolonged PTT ( P < 0.001), reduced maximal extent of vertical laryngeal and hyoid movement compared with non-aspiration patients ( P < 0.001). Whereas OTTs of aspiration patients and non-aspiration patients were similar ( P = 0.412). The patients in the two groups had prolonged OTT compared with control subjects (P < 0.001). Maximal extents of anterior laryngeal (P = 0.215) and hyoid (P = 0.168) movement of the subjects in the three groups showed no differences. The relationship of kinematic parameters and aspiration On logistic regression analysis the important independent predictors of aspiration were prolonged PDT, prolonged PTT, reduced maximal extent of vertical laryngeal movement and reduced maximal extent of vertical hyoid movement [Table - 5]. Discussion Penetration-aspiration is a common swallowing abnormality in post-stroke patients and should be identified accurately to facilitate the management strategies for dysphagia. The combined consequence of dysfunctions such as impaired epiglottic eversion, pharyngeal paralysis, and incomplete laryngeal elevation result in inefficient bolus transit and impaired airway protection. In this preliminary study VFSSs were done to identify the differences between stroke patients and healthy subjects in kinematic parameters and P-AS score. Previously very few studies [13] have investigated the associations between kinematic parameters and dysphagia. In this study post-stroke patients had significantly higher scores on P-AS scale when compared to normal subjects. Most swallows performed by the normal subjects scored 1. Though the P-AS showed no aspirations in normal healthy subjects, 15 VFSSs of the 12 normal subjects showed entry of materials into the airway. However, it remained above the level of the vocal folds with clearing suggesting mild penetration. This finding may be due to age-related changes in the oropharyngeal swallowing mechanism or its neural control. In previous studies, age-related changes in aspiration [14] and swallowing duration [15] have been reported. The age-related mild changes in swallowing on VFSS should be differentiated from those caused by neurological disorders. This study showed the differences in the characteristics of patients with and without aspiration. However, it is possible that the small sample size might have either over estimated or under estimated the differences. In our study the side and the location of the lesion had no effect on the occurrence of aspiration. Earlier studies have suggested that dysphagia may be associated with diffuse lesions and lesions in one or both hemispheres, posterior fossa and brainstem. Swallow has a bilateral cortical representation but with consistent interhemispheric asymmetry. [16] This probably explains why some patients develop dysphagia and others do not with similar lesion location. Further observations with more recruits and more detailed classification of the lesion locations are needed. The primary goal of kinematic research is to investigate the differences in kinematic parameters between the healthy population and post-stroke patients with dysphagia. It has been well established that airway protection during swallow requires coordination of bolus flow with the appropriate movements of related structures which protect the airway and propel the bolus through the oropharynx and cervical esophagus. In our study, aspiration was found to be associated with prolonged PTT and PDT. In healthy people, the initiation of laryngeal ascent consistently precedes the arrival of bolus at the hypopharynx. [17] Recent studies showed that post-stroke patients with the longest delays had the most severe aspiration. [17],[18] It has been reported that the prolonged PDT, PTT in stroke patients were the most important temporal determinants of aspiration and closely related to the occurrence of aspiration pneumonia. [10],[19],[20],[21] Pharyngeal delay increases the risk of pre-swallow aspiration. It is not clear to what extent a swallow response should be so delayed that significant swallowing symptoms such as penetration-aspiration in individuals with dysphagia could be caused. As for the spatial parameters, aspiration was associated with reduced maximal extent of vertical laryngeal and hyoid bone movement. We chose the hyoid bone and laryngeal movement for kinematic analysis due to their readily visibility in VFSS and their important role in the swallowing mechanism. [22],[23] It has been suggested that the vertical movement of the hyoid is primarily associated with the closure and protection of the laryngeal vestibule and that the anterior movement is mainly associated with the pulling motion on the cricopharyngeus that allows its opening within the upper esophageal sphincter Upper esophageal sphincter (UES). [22] All the mechanisms discussed above indicate that the measurement of excursions of the hyoid bone as a possible method for the diagnosis of dysphagia. Kuhl [23] observed that laryngeal elevation was reduced in patients with neurogenic dysphagia when compared with healthy subjects. Reduced laryngeal elevation prevents adequate pharyngeal clearance, and the consequent residue may be aspirated after the swallow. However, the neurogenic dysphagias in the patients in Kuhl′s study were due to different etiologies. Though many of the physiological components of swallowing are well understood, current knowledge is incomplete in regard to the temporal-spatial movement during deglutition. It is important to observe the temporal-spatial measures of the movement during swallows because the swallow measures can help to investigate oropharyngeal swallowing physiology objectively and thus allow us to accurately identify the swallow abnormalities resulting in poor airway protection. The method proposed in this study acts as a quantitative approach for the evaluation of swallowing dysfunctions, especially for penetration-aspiration, and helps to understand the complexity of the swallowing process in individuals with and without neurological impairment. We can also postulate that if some kinematic parameters are the predictors of aspiration, management of these factors may help to reduce or even prevent the occurrence of post-stroke aspiration. For example, according to the results of our study, the Mendelsohn maneuver, [24] which is based on the volitional prolongation of the anterior-superior larynx movement, may be helpful for the aspirators with reduced movement of larynx. In summary, the P-AS, combined with fluoroscopic imaging, provides a quantitative method to determine the occurrence of swallow-related airway invasion. It appears promising for the potential contribution to "profiling" abnormal airway-related swallowing events. References
Copyright 2010 - Neurology India The following images related to this document are available:Photo images[ni10009t1.jpg] [ni10009t3.jpg] [ni10009t5.jpg] [ni10009f1.jpg] [ni10009t4.jpg] [ni10009t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}