 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 58, No. 1, January-February, 2010, pp. 48-52 Original Article Demographic and historical backgrounds of the elderly with nonepileptic seizures: A comparative study Goksemin Acar, 1 Martin C. Salinsky Department of Neurology, Pamukkale University, Denizli, Turkey, Correspondence Address: Dr. Goksemin Acar, Department of Neurology, Pamukkale University Medical School, B-103, Kinikli Kampus - 20020, Denizli, Turkey, goksemind@yahoo.com Date of Acceptance: 12-Jan-2010
Code Number: ni10010 DOI: 10.4103/0028-3886.60396 Abstract Background : Non-epileptic seizures (NES) are not infrequent
in the elderly. However, the data on NES in the elderly is likited. Keywords: Demographic, elderly, nonepileptic seizures, psychiatric features Introduction Nonepileptic seizures (NES) are episodes of altered movement, sensation or experience similar to epileptic seizures (ES) but not associated with paroxysmal neuronal discharges. The reported prevalence rates vary between 2 and 33 casesper 100,000 [1] and the average annual incidence for persons over 15 years of age is 1.4 per 100,000. [2] Among patients admitted to epilepsy monitoring units (EMU) the incidence of NES is reported to be 10-20%. [3],[4] NES are most common in young adults. However, the issue of seizures and epilepsy in the elderly has received increased attention only in the recent years due to the growing size of this segment of population. [4],[5],[6] The underlying etiology of NES is either physiological or psychogenic. The proportions of physiological and psychogenic NES differ between young adult and the elderly. The frequency of physiological NES is reported to be 43-50% of the NES in elderly patients as compared to 5-10% of younger patients. [7],[8] Although demographic and historical features of young patients with NES are very well defined, [9],[10],[11],[12],[13] there is limited information about elderly patients with NES. In the tertiary epilepsy referral centers, 10-40% of inpatients are elderly. [8],[14],[15] In retrospective reviews, 9.6-17% of patients over 60 years of age admitted to an EMU were diagnosed as having psychogenic NES. [16],[17] This study is a detailed demographic and historical background review of patients aged 55 years and above with NES in comparison with younger patients. It also details their psychiatric profile and drug use. Materials and Methods This is a retrospective case control study of patients referred to the epilepsy monitoring unit (EMU) of the Oregon Health and Science University and Portland VA Medical Center for differential diagnosis of epileptic and NES and in whom the diagnosis of NES was confirmed by long term video EEG. The diagnosis of NES used the following criteria: [18] 1) Two or more seizures recorded during video EEG monitoring, which were typical of the habitual seizures; 2) No abnormal epileptic discharges in EEG before, during and after the seizure; 3) Seizure appearance consistent with NES and not consistent with ES. Patients with purely subjective spells or unilateral motor activity without alteration of consciousness were excluded. Patients with documented ES or with interictal epileptiform abnormalities were also excluded. All patients admitted to our EMU from 1999-2006 were screened. Following the determination of patients with NES over 55 years of age, the next two consecutive subjects between 18-45 years of age who were meeting inclusion criteria in our database were selected as controls for each elderly subject. Video and EEG recordings of all spells were reviewed to confirm the diagnosis. For all cases meeting the inclusion criteria, chart review included:
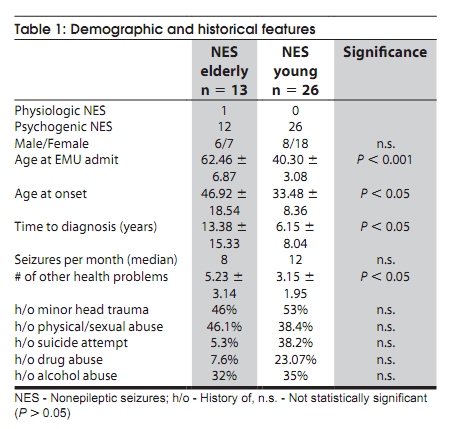
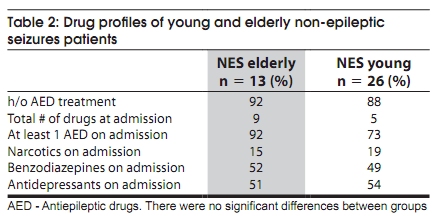
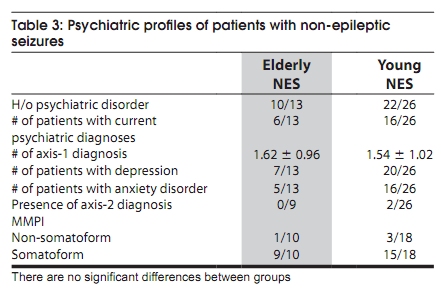
The results of MMPI-2 testing were categorized as somatoform, or non-somatoform using previously published criteria. [19] Statistical analysis Nonparametric tests were used to compare two independent samples since the data was not normally distributed. Chi square test was performed for nominal variables. Results Demographic and historical features Of the 469 patients admitted for long term video-EEG monitoring, 128 (27%) patients wer diagnosed to have pure NES. In the total cohort of 469 patients, 78 (16.7%) patients were over 55 years of age and 14 (17.9%) of them had pure NES. The video record of one patient was not available for review. Data of these 13 patients with NES were analyzed and compared to the data of 26 patients with NES aged between 18 and 45 years. Of these 13 patients, only one had physiological NES due to a combination of low blood pressure, tachycardia and fixed stenosis of one internal carotid artery. In the young group none of the patients had physiological NES. Demographic features are summarized in [Table - 1]. The length of time between the onset of NES and diagnostic EMU admission was much longer in the elderly group as compared to the young group (P < 0.05). Seizure frequency within three months prior to admission was eight per month in the elderly group and 12 per month in the younger group (NS). The male to female ratio was more evenly distributed in the elderly as compared to the young group, though the difference did not reach statistical significance. Past medical/Psychosocial history The history of physical or sexual abuse was recorded in 46.1% of the elderly and 38.4% of the younger patients. Nearly half of each group (46% of the elderly; 53% of the young) was exposed to minor head trauma (defined above). The number of health problems within the past five years was higher in the elderly group (P < 0.05) [Table - 1]. History of antiepileptic drug (AED) use was present in 92% of elderly patients with NES and 88% of the younger patients with NES. The mean total number of prescription drugs at the time of admission was five for the younger group and nine for the elderly group. At admission 92% of the elderly and 73% of the younger were on at least one AED. At least one narcotic drug was prescribed for 15% of the older and 19% of the younger patients. Benzodiazepines and anti-depressant drugs were prescribed in almost half of the patients in both groups [Table - 2]. History of a psychiatric disorder was present for a great majority of the patients in both the groups [Table - 3]. A history of suicide attempt was higher in the younger group. History of drug abuse was higher in the younger patients (23.07% vs. 7.6%; n.s.). The history of alcohol abuse did not differ between the two groups. Psychological evaluation and minnesota multiphasic personality inventory results Most of the patients had one or more psychiatric diagnoses made at the time of EMU admission. The number of axis-1 diagnosis did not differ between the groups [Table - 3]. The most common diagnosis was depression (7/13 in the elderly, vs. 20/26 in the younger patients). The second most common diagnosis was anxiety disorder. Two patients in the younger group had an axis-2 diagnosis, both were borderline personality disorder. There were no axis 2 diagnoses in the elderly group. MMPI test results were available for 10 of 13 elderly and 18 of 26 younger patients. Nine out of the 10 elderly (90%) and 15 out of 18 younger (83%) patients had a profile consistent with a somatoform disorder. [19] Seizure semiology The video record reviews included at least three spells. Provocative procedures were not used during any of the spells. The major behavioral characteristics were tremulous or shaky extremity movements with a waxing and waning pattern, rocking of the body back and forth, biking, pelvic thrusting, thrashing movements of the arms/legs/head, cheek biting, bizarre dystonic posturing. Majority of the patients lost responsiveness or very slow in obeying commands. A few patients complained of breathlessness. Self injury, tongue biting or incontinence was not observed. Discussion In this series, 27% of all patients admitted to our tertiary epilepsy referral center had pure NES. Of all NES patients 10.9% were over 55 years of age, similar to the 9.6% reported in an earlier study. [17] Of the elderly patients admistted to our EMU, 18% were diagnosed to have pure NES, a percentage similar to that reported by McBride et al.[7] and somewhat lower than the 44% reported by Kellinghaus et al. [8] It can be concluded that NES are not uncommon among elderly patients. We found some differences between younger and older NES patients. Most important difference was that older NES patients had a significantly longer delay between the onset of spells and referral for diagnostic video EEG monitoring. This delay may reflect physicians′ inclination to accept spells in the elderly without investigation. Spells in the elderly may be overshadowed by other health complaints. Physical and social impairment due to refractory episodes may be perceived more threatening in younger patients, leading to earlier diagnostic investigation. These long delays in referral (averaging 13 years) result in sustained disability and for many patients long-term unnecessary exposure to AEDs, AED side effects, and potential drug-drug interactions. We also found a gender difference between the age groups. In younger psychogenic NES patients women outnumber men by a substantial margin. [1],[2],[10] We found a more even sex distribution in our older patients. A majority of patients in both the groups had a history of at least one AED trial, and most were on AEDs at the time of admission. Kellinghaus et al. reported that 12 of 17 elderly patients with NES were on an AED at admission. [8] Drury et al. reported similar observation. [14] It is also worth noting the frequent use of narcotics and benzodiazepines, possibly related to the common association of psychogenic NES and somatoform disorders. Antiepileptic drugs, narcotics and benzodiazepines may all contribute to neurotoxic effects. This is particularly important in the elderly. In this age group pharmacokinetics may be altered due to multiple drug combinations and decreased hepatic and renal clearance. Our results support the need for early diagnosis with video-EEG, especially in the elderly, in order to avoid the potential risks associated with AEDs and combined therapies. Previous studies have noted that a history of physical or sexual abuse was frequent in patients with psychogenic NES. [13, 20, 21] In a prospective study Westbrook et al. reported that 32% of patients with psychogenic NES between 15- 55 years of age had a history of abuse. [22] This appears to be true of older patients as well. 46% of older patients and 39% of younger patients reported such abuse in our series. A history of minor head trauma has been reported in 21-33% of psychogenic NES patients. [22- 24] We found similar (but higher) percentages in both the groups (46% in the elderly, 53% in the younger group). As expected, the number of health problems was higher in the elderly. Psychiatric diagnoses are common in psychogenic NES patients. [20],[23] A history of psychiatric disorder was found in about 90% of our elderly patients. The most common diagnosis was depression followed by anxiety disorders, consistent with the previous reports. [20],[23],[25],[26] The MMPI of both older and younger groups revealed a somatoform profile in most patients, consistent with previous observation. [19] We found a higher percentage of younger patients than the elder patients had a history of suicidal attempt. Suicidal ideation and attempt is common among younger NES patients. [26] Conclusion Psychogenic NES is a common disorder which is frequently misdiagnosed as epilepsy and treated with AEDs. Our results in a group of elderly psychogenic NES patients suggest that older patients do not differ from the younger patients in terms of most demographic and historical features, but the diagnosis is significantly delayed, often by more than a decade. During this time the potential toxic effects of AEDs accrue and appropriate psychiatric treatment is not obtained. The diagnosis of psychogenic NES should be considered in elderly seizure patients whenever atypical historical or clinical features are present, or in the setting of coexistent psychiatric disorder. Prompt referral for diagnostic monitoring may reduce the long-term disability associated with this disorder. Acknowledgment This study was supported by The Scientific and Technological Research Council of Turkey. References
Copyright 2010 - Neurology India The following images related to this document are available:Photo images[ni10010t1.jpg] [ni10010t2.jpg] [ni10010t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}