 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 58, No. 1, January-February, 2010, pp. 58-61 Original Article Effect of early treatment in polymyositis and dermatomyositis Peyman Naji, Farhad Shahram, Abdolhadi Nadji, Fereydoun Davatchi Rheumatology Research Center, Tehran University of Medical Sciences, Tehran, Iran Correspondence Address: Dr. Farhad Shahram, Rheumatology Research Center, Shariati Hospital, Kargar Avenue, Tehran - 14114, Iran, shahramf@tums.ac.ir Date of Acceptance: 02-Jul-2009
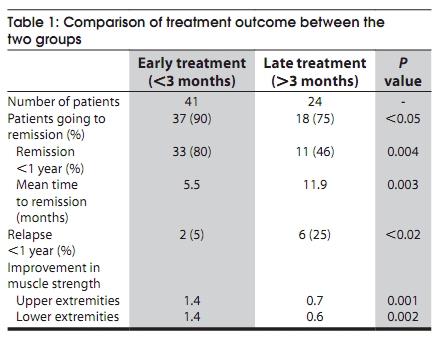
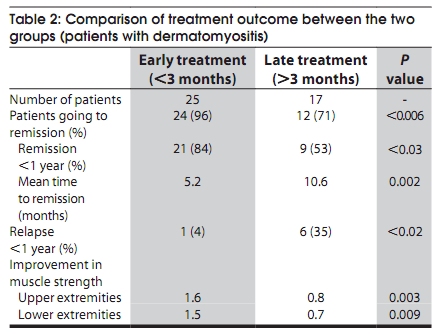
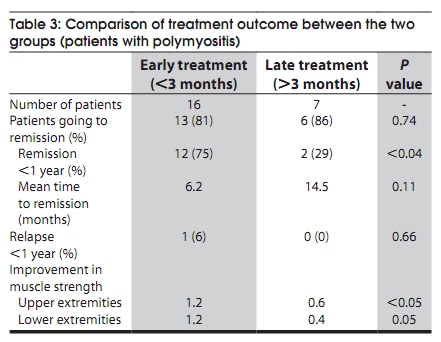
Code Number: ni10012 DOI: 10.4103/0028-3886.60398 Abstract Background : Idiopathic inflammatory myopathies, dermatomyositis (DM) and polymyositis (PM) are rare but are potentially treatable. Keywords: Dermatomyositis, early treatment, inflammatory myositis, polymyositis, relapses Introduction Idiopathic inflammatory myopathies are rare conditions, with an estimated prevalence of 0.5 to 9.3 cases pers million. [1] The main goal of therapy in these conditions is to improve muscle strength and function in activities of daily living, as well as to ameliorate extra-muscular manifestations. [2] Due to lack of randomized controlled clinical trials and evidence-based data, treatment of idiopathic inflammatory myopathies still remains empirical. [1] Most authorities recommend use of corticosteroids as the first-line drug for polymyositis (PM) and dermatomyositis (DM), which has been shown to be quite effective. However, nearly 30% of the patients will eventually need other immunosuppressive drugs, because of resistance to corticosteroids, side-effects or difficulties in tapering the dose of steroids. [2],[3],[4],[5] In a study on the influence of clinical variables on the muscle strength improvement in patients with PM and DM it has been shown that an early treatment is associated with a favorable response. [4] In view of high morbidity and mortality associated with PM/DM, Marie et al., emphasized the importance of treating these patients at an early stage. [5] Early treatment with immunosuppressive drugs and better medical care is associated with improved survival rates in patients with PM/DM. [6] In an outcome study in juvenile DM, Chowdhary et al. recognized the importance of early and aggressive treatment for improved outcomes. [7] In the study by Tymms and Webb, the outcome was worse in patients with duration of the disease more than four months before diagnosis. [8] In the nationwide study in Finland, the predictive factors for long-term outcome, death were age for both PM/DM group and the delay in the diagnosis for PM group. [9] The aim of this study was to compare the effect of early and late treatment in patients with PM and DM. Materials and Methods The study cohort included all adult patients with definite diagnosis of PM or DM (according to Bohan-Peter criteria) [3] treated for at least 12 months. Patients less than 16 years old and patients with other rheumatologic disorders (overlap syndromes) or malignancy were excluded. Patients in the later groups were excluded as the type of treatment prescribed in these patients largely depends either on the underlying disease (for example, combination chemotherapy for malignancies) or other organ involvement (kidney, lungs, etc. in cases of overlap syndromes) and such treatments might influence the treatment outcomes independent of the duration of the disease. All patients were treated with prednisolone (1 mg/kg body weight daily) alone or in combination with oral methotrexate (10 to 15 mg weekly) or azathioprine (2-3 mg/kg body weight daily). They were divided into two groups: Early Group - treatment within three months of onset of disease and Late Group - treatment after three months of onset of disease. Patients were follow-up every month for the first six months, every two months for the second six months and then every two or three months thereafter. During each visit a complete physical examination including muscle force and muscle enzymes were recorded. Muscle strength was tested by manual muscle test method on a five-grade scaling. Muscle groups tested were shoulder abduction (deltoid middle) and biceps brachii in the upper extremity, and knee extensors (quadriceps), gluteus maximus and gluteus medius in the lower extremity. The follow-up data of all the patients in both groups were recorded. This was also done separately for patients with PM and DM. At the initial visit patients were graded to have severe disease if the muscle strength was less than grade 3/5 in either upper or lower extremities, and/or cardiac (myocarditis, congestive heart failure, arrhythmia, or decreased left ventricle ejection fraction) or pulmonary (dyspnea, cough, or interstitial changes in chest radiographs) involvement were present. The time of onset of either proximal muscle weakness clinically or characteristic skin manifestations was considered for calculating the disease onset. Disease remission was defined as normalization of creatine kinase (CK) level, improvement of proximal muscle strength and improvement or at least no deterioration in the extra-muscular involvements. Improvement of proximal muscle strength was defined as either an increase of at least two grades in muscle force (on a five-grade scaling) or reaching muscle force to 4/5 regardless of the initial score, observed in both upper and lower extremities. We considered dysphagia, regurgitation, nasal speech and joint involvement as other extra-muscular involvements. Going to remission in less than one year after the treatment was considered as "positive therapeutic response". The number of patients with positive therapeutic response and the mean time elapsed for reaching the remission were assessed and compared between the two groups. We also determined the effect of severity of the disease on therapeutic response. Chi-square test, Fisher′s exact test, t-test and Pearson correlation test were used for data analysis using SPSS (Version 11.5) software. Results Of the cohort of 185 patients with PM/DM registered during the past 15 years, 65 patients (44 female, 67.7%) met the inclusion and exclusion criteria. Forty-two patients had DM (28 female, 66.7%) and 23 had PM (16 female, 69.6%). The mean age of the patients was 34.5 ± 11.3 years, 37.8 ± 13 for patients with PM and 32.6 ± 10 for patients with DM. Severe form of the disease was seen in 32.3% (21 patients; seven in the PM group and 14 in the DM group), whereas 44 patients had mild form of the disease (16 in the PM group and 28 in the DM group). Extra-muscular involvement was seen in 55.4% (36 patients; 11 in the PM group and 25 in the DM group). Late Group included 24 patients (36.9%, seven with PM and 17 DM), while Early Group included 41 patients (63%, 16 with PM and 25 with DM). Two methods of treatment were employed, 15 patients in the Late Group and 20 patients in the Early Group received prednisolone alone, while nine in the Late Group and 21 patients in the Early Group received combination therapy. The difference was not statistically significant (P = 0.42). Delay in treatment had an affect on the therapeutic outcomes with statistically significant difference [Table - 1]. Remission rate was higher in Early Group (90 vs. 75%, P < 0.05), notably when comparing those going to remission in the first year of treatment (80 vs. 46%, P: 0.004). The mean time needed to go to remission was much less with early treatment (5.5 vs. 11.9 months, P: 0.003). The relapse rate (less than one year after remission) was also lower in Early Group (5 vs. 25%, P < 0.02). Improvement in muscle strength showed a significant difference between Early and Late Groups both in upper (1.4 vs. 0.7 on 5, P: 0.001) and lower extremities (1.4 vs. 0.6 on 5, P: 0.002) at one year after treatment [Table - 1]. There was significant relation between the delay in starting treatment and the time for achieving remission ( P < 0.00001, Pearson correlation coefficient: 0.522); the higher the gap, the longer the time elapsed to go into remission. There were three deaths (two with PM and one with DM) and all of them in patients with severe disease. It was interesting to note that none of them were in the delayed treatment group ( P: 0.52). The comparison of treatment outcome showed the same significant results in those with DM [Table - 2], while the delay in treatment showed no statistically significant difference in remission or relapse rate or mean time to go to remission in patients with PM. However, positive therapeutic response (75 vs. 29 percent, P < 0.04), and improvement in muscle strength (75 vs. 29%, P < 0.04) was higher in patients with PM [Table - 3]. The relation between the delay in starting treatment and the time needed for going to remission was significant in both DM (P: 0.005, Pearson correlation coefficient: 0.460) and PM patients (P < 0.02, Pearson correlation coefficient: 0.563). Discussion Our results show that early treatment, within the first three months of disease onset in patients with PM and DM improves the remission rates, shortens the time needed to achieve remission, maintains the muscle strength and reduces the relapse rate, notably in patients with DM. Similar were the observations in the study by Tymms and Webb, in this study patients receiving treatment within four months of onset of symptoms had higher rate of good response when compared to patients receiving delayed treatment (72 vs. 21%). [8] Our study also showed that delayed treatment was associated with achieving late remission. Similar were the conclusions in the earlier studies. [1],[5] In our study, patients with DM showed better results with early treatment. This effect was also observed by Fafalak et al.,[5] but the difference was not statically significant. Patients receiving early treatment showed higher muscular force within six months after starting therapy, in both Fafalak et al. study [5] and the present study. In regard to mortality, better outcome had been shown by early treatment in several studies. [5],[6],[9] In our study all the three deaths were in the Early Group and it was probably related to the severity of the disease. Conclusion Early diagnosis and early institution of appropriate drug treatment in patients with PM/DM are associated with better therapeutic response, shorter treatment interval and reduced complication rates. References
Copyright 2010 - Neurology India The following images related to this document are available:Photo images[ni10012t2.jpg] [ni10012t1.jpg] [ni10012t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}