 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 58, No. 1, January-February, 2010, pp. 62-68 Original Article Evolution of endovascular management of intracranial dural arteriovenous fistulas: Single center experience Rashmi Saraf, Manish Shrivastava, W. Siddhartha, Uday Limaye Department of Radiology, Division of Interventional Neuroradiology, KEM Hospital, Mumbai, India Correspondence Address: Dr. Uday Limaye, Department of Radiology, Division of Interventional Neuroradiology, KEM Hospital, Mumbai - 400 012, India, udaylimaye123@gmail.com Date of Acceptance: 22-Dec-2009
Code Number: ni10013 DOI: 10.4103/0028-3886.60400 Abstract Aim : We aim to focus on the treatment of intracranial dural
arteriovenous fistulas (DAVF) with emphasis on the evolution of endovascular
management at our center over the last 13 years. We also aim to highlight
the present treatment strategy, considering all the embolic agents available
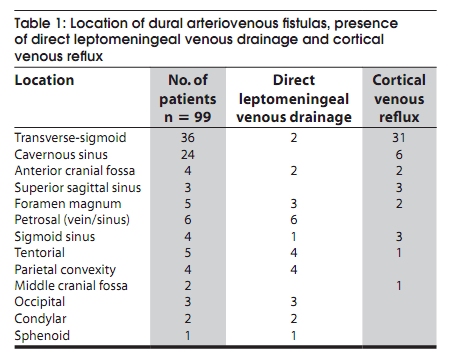
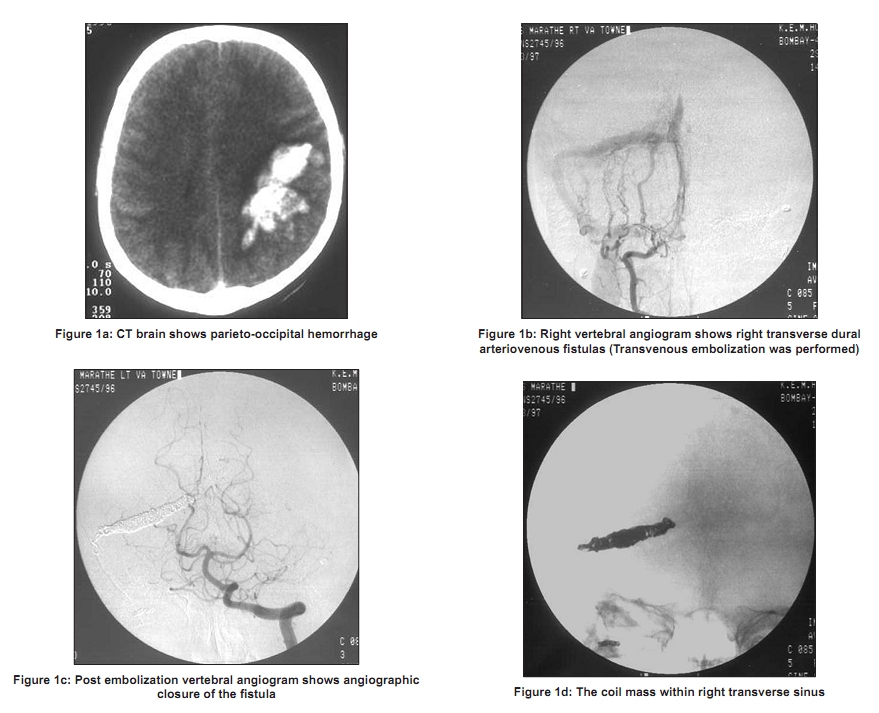
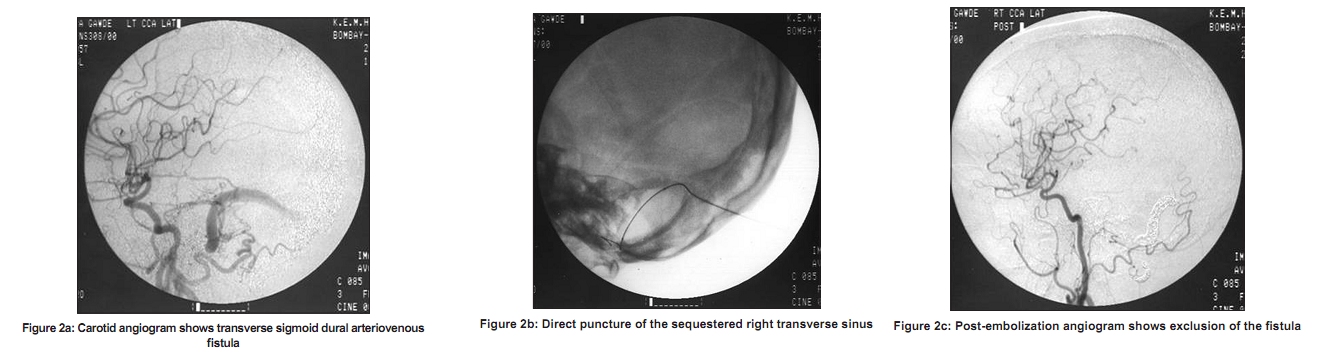
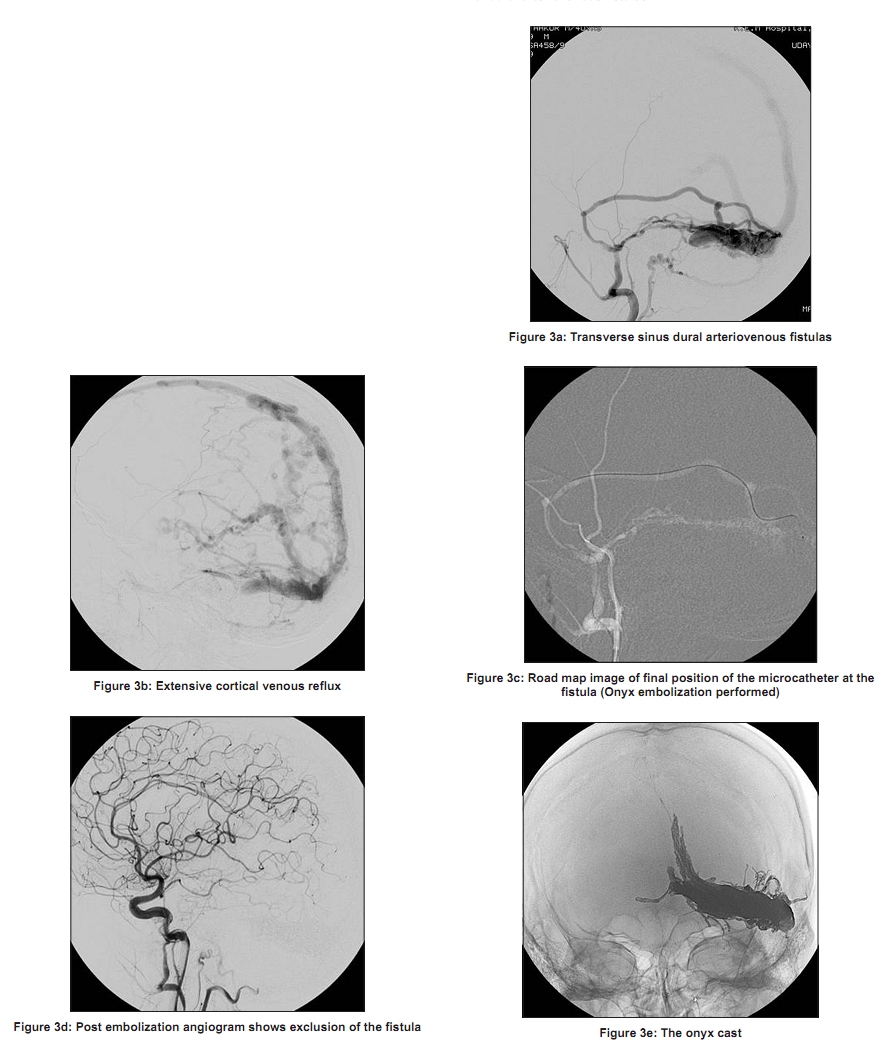
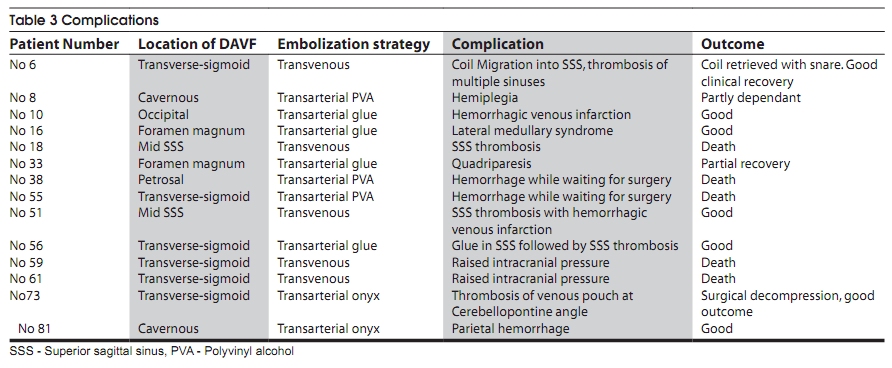
with us. Keywords: Dural Arterio-venous fistula, embolization, Onyx Introduction Intracranial dural arteriovenous fistulas (DAVFs) are complex vascular lesions which often present with intracranial hemorrhage. [1] Selected studies suggest that they account for 10-15% of all intracranial arteriovenous lesions. They are acquired lesions. Venous thrombosis is the most common predisposing factor. [2] Venous thrombosis induces opening of microscopic shunts in the wall of the thrombosed sinuses, which progress to the formation of direct fistulous connections between the dural arteries and the sinuses or the cortical veins. [3],[4] The clinical presentation of DAVFs is variable and shows strong correlation with the venous drainage pattern. The presence of cortical venous drainage or reflux is the weak point of these lesions which leads to intracranial hemorrhage. [5] Prompt and definitive treatment is needed for these lesions. Embolization has been the mainstay of treatment. Through this study we aim to focus on the treatment of intracranial DAVFs with emphasis on the evolution of endovascular management at our center over the last 13 years. The treatment philosophy has undergone gradual change over time. Literature search has shown limited Indian data on the endovascular management of DAVFs. We present the largest case series of endovascular management of DAVFs in India (comprising of 99 patients). The treatment preferences have gradually changed from transarterial polyvinyl alcohol (PVA) particles to transvenous coiling, transarterial glue to transarterial embolization with injection Onyx. This is an attempt to analyze the evolution to propose a treatment strategy which will lead to higher cure rates with reduced complications. Materials and Methods Patients This is a retrospective study of 99 patients of DAVFs seen from December 1995 to March 2009. Seven patients were found to have spontaneous thrombosis after diagnostic angiography. The other 92 patients underwent endovascular treatment. There were 63 males and 36 females with ages ranging from one month to 68 years and an average age of 44. Among these, three were infants (less than 10 months) with dural sinus malformation. Location of the DAVFs and the presence of direct leptomeningeal venous drainage (DLMVD) and cortical venous reflux (CVR) are shown in [Table - 1]. History of sinus thrombosis was present in 15 patients and nine had prior history of trauma. Thirty eight patients presented with hemorrhage, of which 87% (33) had cortical venous drainage. Twenty eight patients (28.2%) had DAVFs, which drained directly into the leptomeningeal veins of which 79% (22) presented with hemorrhage. 49 patients (50%) had cortical venous reflux. 11 patients had sequestered sinus of which majority (nine) were in transverse-sigmoid sinus. Clinical Presentation Intracranial hemorrhage was present in 38 out of 99 patients (38%). Thirty three of these 38 had either cortical venous reflux or direct leptomeningeal venous drainage. Ocular signs and symptoms (proptosis, congestion, cranial nerve palsy without decrease in visual acuity) were present in 31 patients of which 24 were DAVFs of the cavernous sinus. Other presentations were neuropsychiatric symptoms, tinnitus, altered sensorium, loss of consciousness and seizures. Multiple DAVFs were seen in two patients. Treatment Strategy The current aim of treatment in DAVFs is cure, which is achieved by occlusion of the vein of the fistula. The vein of the fistula may be a sinus or a leptomeningeal vein. The best access which leads to the fistula and the vein to be occluded is selected. At the beginning of our experience, we only used the transarterial access to achieve preoperative embolization or palliation. The preference changed to transvenous access from 1998 up until 2006. The sinus was intentionally occluded in order to achieve cures. The DAVFs on the sequestered sinuses were treated by transosseous routes. Access to the sinus was achieved with a direct puncture through a burr hole made prior to the procedure. About 79% cure was achieved in 33 patients by transvenous embolization. However, DAVFs on leptomeningeal veins were still treated transarterially using glue to reach the vein through the fistula. Since 2006, Onyx has been the embolic agent of choice for all types of DAVFs except those on cavernous sinuses for which the transvenous route is still used. Onyx is a nonadhesive liquid embolic agent comprising of an ethylene vinyl alcohol (EVOH) copolymer dissolved in DMSO (dimethyl sulfoxide) and suspended micronized tantalum powder to provide contrast for visualization under fluoroscopy. Onyx is available in two product formulations, Onyx 18 (6% EVOH) and Onyx 34 (8% EVOH). In total, PVA embolization was done in four patients, transvenous coiling in 33, transarterial glue only in 15 and direct puncture for sequestered sinus in four. Thirty six patients underwent transarterial Onyx embolization. Results A total of 99 patients of DAVFs have been studied from December 1995 to March 2009. Seven patients had spontaneous thrombosis after diagnostic angiography. The results are presented depending on the routes of embolization. [Table - 2] shows the access, cure rates and complication rates. Ninety patients were treated by embolization alone and two were treated in combination with surgery. Both had undergone prior transarterial particle embolization. Combined cure rates and complication rates of the non Onyx group (56 patients) were compared with those of the Onyx group (consecutive 33 patients from 2006 to 2009). The cure rates were significantly higher in Onyx group (Chi square test P value .007) and the complication rates significantly lower (Chi square test P value .038) as compared with non Onyx group. Transarterial embolization was performed using PVA particles in the first four patients of our series. Two patients were cured. DAVFs with direct leptomeningeal drainage (28 patients) have been treated with transarterial Glue(15) or Onyx (13). Complete cure was obtained in all 28 patients. Transvenous embolization was performed in 33 patients. Coils and Glue were used for the same. 17 patients in this group had DAVFs of the cavernous sinus and cure was achieved in 15. Ten patients had transverse-sigmoid DAVFs with cure in 7 patients and complications in 2 of them [Figure - 1]. Direct puncture was performed in four patients with isolated transverse sinuses through a burr hole. This was followed by packing of the sinus with coils and Glue. Cure was achieved in all. [Figure - 2] Onyx Embolization: Transarterial embolization with Onyx was started in 2006. Onyx embolization was done in 36 patients of DAVFs. Angiographic cure was achieved in 33. (Cure rate of 92%) [Figure - 3] 11 of the 36 patients had direct drainage into leptomeningeal veins and seven patients had a sequestered transverse sinus. Cure was achieved in all 11 patients. The angiographic cures had been reconfirmed after six months on follow-up angiograms. with use of Onyx, the cure rates have improved to 92% (33/36) as compared to the combined cure rates of the non Onyx group which was 84% (47/56) The non Onyx group included PVA embolization (four patients), transvenous coiling (33 patients), transarterial Glue (15 patients) and transosseous embolization for sequestered sinus (four patients). Complications In the entire series we encountered 14 complications. [Table - 3] elaborates them. Twelve of these (five deaths) occurred in 56 patients prior to the use of Onyx (complication rate of 21%). These were due to sudden changes in the intracranial hemodynamics leading to hemorrhage, venous infarctions or raised intracranial pressure. In the Onyx group, there were two complications out of 36 patients (no deaths). This is significantly lower as compared to previous embolic agents. (P value equals 0.038). Discussion Dural AVFs are uncommon intracranial vascular lesions comprising of direct, abnormal connections between the meningeal arteries and the dural venous sinuses or leptomeningeal veins. DAVFs are acquired lesions with venous sinus thrombosis being the predominant predisposing factor. [6],[7] Pediatric DAVFs are rare lesions and are considered to be congenital. [8],[9],[10] A multitude of studies have proven that the aggressive ness of DAVF has strong correlation with presence of cortical venous drainage from the fistula. [8],[9],[10] DAVFs with isolated sinus and direct leptomeningeal venous drainage are extremely aggressive lesions. [11],[12] In our series, 87% of the patients who presented with hemorrhage had cortical venous drainage. Aggressive clinical features include focal neurological deficits, seizures, intracranial haemorrhage, papilledema, memory disturbances or myelopathy. [12],[13],[14],[15],[16] Spontaneous thrombosis of DAVF after diagnostic angiography and multiple DAVFs are well known in literature. [17],[18],[19] In our study, dural sinus thrombosis was the most common predisposing factor. Seven patients had spontaneous thrombosis after diagnostic angiography. Multiple DAVFs were seen in two patients. Transverse-sigmoid sinus was the commonest site and intracranial hemorrhage was the most common presentation. 92% of the patients of transverse-sigmoid sinus DAVF had cortical venous reflux and all who presented with hemorrhage had cortical venous reflux. Seventy nine percent of the patients with DAVF, leptomeningeal venous drainage presented with hemorrhage. DAVFs thus are life threatening complex lesions, very often requiring urgent definitive treatment. [20],[21] Surgery can be hazardous considering the transosseous arterial supply, high flow and engorged veins or sinuses. [22] Radiosurgery series have reported mixed outcomes. [23],[24],[25] Embolization has been the mainstay of treatment of patients with DAVFs at our center. In our experience, we achieve safe and durable cure of a DAVF, when we embolize the first draining vein of the fistula which may be dural venous sinus or a cortical vein. The endovascular access (transarterial/transvenous/direct puncture), which got us closest to the target (the first draining vein) and gave high chance of cure, was chosen for each patient. Evolution of endovascular treatment has had a close association with improving catheter technology, better understanding and innovative treatment philosophy. It has undergone a full circle, starting from transarterial to transvenous and the returning to the transarterial option (with Onyx). The treatment strategies too have undergone gradual but definite change over the period of last decade. In the initial years, the aim of endovascular treatment was preoperative reduction of vascularity or for palliation of symptoms. This was done by particle embolization or occlusion of feeding arteries. [26] Transarterial embolization with particles generally does not lead to permanent cure. Two of our patients who had transarterial particle embolization suffered fatal hemorrhages while waiting for surgical treatment. Transvenous embolization of DAVFs (with coils and glue) achieved cure by endovascular treatment in 79% in our series [Figure - 2]. However, these were prolonged procedures requiring large number of coils and with unpredictable outcomes and high complication rates. There is considerable literature on transvenous embolization of DAVFs. [27],[28],[29] DAVFs draining directly into leptomeningeal veins had high cure rates with endovascular treatment. They were treated by transarterial glue or Onyx injections. Complete cure was achieved in all the 28 patients of this group. High cure rates have been reported in literature for these lesions. [30],[31] Transosseous direct puncture of isolated sinuses was done in four patients in our series with 100% cure rate. This technique is well described in literature. [32],[33] We have now switched to Onyx in this subgroup as well, obviating the need for burr holes and transosseous punctures of high flow fistulas. Liquid embolic system Onyx (ev3), with its unique physical properties and excellent endovascular handling allows complete occlusion of the diseased sinus or proximal vein. This can be achieved without reflux into the cortical veins thus minimizing complications. The technique of Onyx injection (plug and push) and its advantages (time to think, slow penetration, ability to fill all the vascular compartments and crevices of the malformation, control over reflux etc) have been well documented. Onyx gives us advantage in achieving the goal of occluding the vein at the end of the treatment. Onyx has been equally effective in all types of DAVFs (those draining into sinus or with direct leptomeningeal drainage or with sequestered sinuses). It has helped achieve high cure rates with safety and durability. [34] Our experience of Onyx in DAVFs has been remarkable leading to a cure rate of 92% in all types of fistulas. Hence we prefer Onyx as the primary treatment modality in DAVFs of all locations except the cavernous sinus. Various studies are now proving the efficacy of Onyx in the management of DAVFs. [35],[36] In cavernous DAVFs, transvenous route is still preferred as there are multiple dangerous arterial anastomoses in that region. Also, a good transarterial access is usually not present. Most cavernous DAVFs will have a good transvenous access. [37],[38],[39],[40] Onyx is used for cavernous DAVFs only if the transvenous access has failed. Only one patient of cavernous DAVF in our series had to be treated with Onyx. The experience with transvenous embolization, transarterial glue and transarterial Onyx has given a better understanding of this disease and has helped us to be in a position to achieve safer and durable cures. Conclusion Cortical venous reflux or drainage is associated with aggressive nature of the DAVFs. Earlier, endovascular procedures were of long duration, done in multiple sessions with incomplete cures and higher complications. With gradual developments in endovascular strategies, technical advances and with better embolic agents, embolization has become the treatment of choice. High cure rates are now expected with embolization, with minimal complications. Transvenous embolization with coils and glue was the mainstay of treatment for many years. We are still employing the transvenous route for Cavernous DAVFs. Glue was also used for DAVFs draining directly into leptomeningeal veins. The advent of Onyx has significantly improved the endovascular treatment of DAVFs leading to higher cure rates compared to transvenous embolizations. It is equivalent to glue for DAVFs with direct leptomeningeal drainage. Complications with Onyx are significantly lesser than previous agents. Currently we propose Onyx as the first choice in endovascular treatment of DAVFs.[41] References
Copyright 2010 - Neurology India The following images related to this document are available:Photo images[ni10013t2.jpg] [ni10013t3.jpg] [ni10013f3.jpg] [ni10013t1.jpg] [ni10013f1.jpg] [ni10013f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}