 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 58, No. 1, January-February, 2010, pp. 74-77 Original Article Quality of life with special respect to depression after surgical treatment of hypertensive basal ganglia hemorrhage Jian Hai, Lin Zhang, Fei Wang, Jue-Feng Wan, Qing-Gang Pan Department of Neurosurgery, Tongji Hospital, Tong ji University, Shanghai - 200 065, China Correspondence Address: Dr. Hal Jian, Department of Neurosurgery, Tongji Hospital, Tongji University, 389 Xincun Road, Shanghai - 200 065, China, haijiandoc@yahoo.com.cn Date of Acceptance: 28-Aug-2009
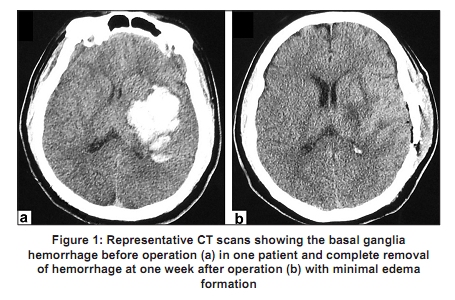
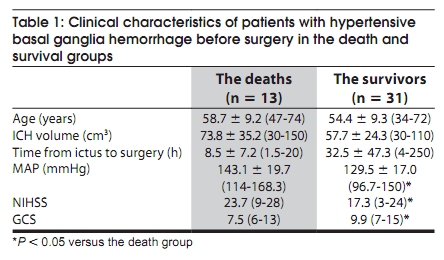
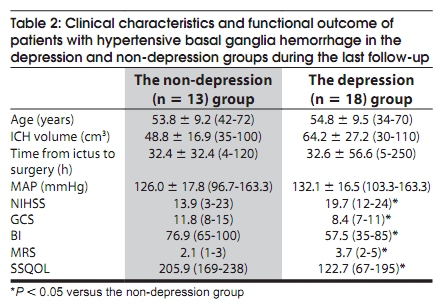
Code Number: ni10015 DOI: 10.4103/0028-3886.60403 Abstract Background : Hypertensive intracerebral hemorrhage is associated with high mortality and morbidity. Place of surgery in the primary supratentorial intracerebral hemorrhage is uncertain and the data on the long-term functional outcome of surgery in these patients is limited. Keywords: Basal ganglia hemorrhage, craniotomy, depression, hypertension, quality of life Introduction Basal ganglia is one of the common sites of hypertensive intracerebral hemorrhage and is associated with a high mortality and severe disability. [1] The place of surgical treatment in hypertensive basal ganglia hemorrhage is uncertain. Theoretical beneficial effects of clot evacuation include: Reduced intracranial volume, lowered intracranial pressure, reduced risk of edema formation, and improved cerebral perfusion [2],[3] However, several randomized studies did not show any outcome or survival benefit after surgical intervention compared to medical treatment. [1],[4],[5] Little is known about the long-term prognosis of patients with hypertensive basal ganglia hemorrhage treated surgically, especially in respect to depression. We studied the long-term functional outcome in patients with hypertensive intracerebral hemorrhage who underwent surgical evacuation and evaluate. Materials and Methods Patients with hypertensive basal ganglia hemorrhage seen between December 2002 and May 2007 were enrolled in this study. A history and examination, including an assessment of the baseline level of consciousness by Glasgow Coma Scale (GCS) [6] and of the neurological status by National Institute of Health Stroke Scale (NIHSS) [7] were obtained at the time of admission. The time of onset of symptoms was determined on the basis of interview of the patient, family or witness. The volume of the intracerebral hemorrhage (ICH) was measured hy the formula ABC/2, where A is the greatest diameter of the hemorrhage by computerized tomography (CT), B is the diameter 90 degrees to A, and C is the approximate number of 10 mm CT slices with hemorrhage. [8] Inclusion criteria included: Hypertensive basal ganglia hemorrhage diagnosed by CT scan, ICH volume> 30 cm 3 with mild to moderate alterations in the level of consciousness (GCS range: 6-12) and age> 18 years at the time of enrollment. Exclusion criteria included: No alterations in the level of consciousness, infratentorial ICH, CT suggestive of underlying structural vascular abnormality such as arteriovenous malformation or aneurysm (presence of subarachnoid hemorrhage), intraventricular hemorrhage, extension of a supratentorial hemorrhage into the brainstem, severe systemic disease, terminal medical illness, coagulopathy, traumatic ICH, pregnancy, failure to obtain informed consent, and patients with severe aphasic and mental disability that might interfere with the assessment of outcome. The mean arterial pressure (MAP) was recorded before operation. The study was approved by the ethics committee of the Tongji Hospital, Tongji University. All patients received conservative treatment according to current practices. Surgical evacuation of ICH was considered in patients who had clinical deterioration inspite of optimal conservative therapy. Informed consent was obtained from the patient or, if the patient could not provide informed consent, from the patient′s legally designated representative. Surgical evacuation consisted of a small-window craniotomy and evacuation of the hematoma under microscopic illumination and magnification. The intention of surgical treatment was complete removal of the clot and to control elevated intracranial pressure [Figure - 1]. For functional outcome evaluation Barthel Index (BI) [9] and modified Rankin Scale (mRS) were employed. [10] A BI of $60 or a mRS < 4 was defined as good functional recovery. [11] Depression was assessed with Beck Depression Inventory (BDI), which is a self-evaluation 21-question-survey and a score> 9 indicates depression. [12] Quality of life was measured with the stroke-specific quality of life (SSQOL) scale. [13] This scale consists of 49 items in the following domains: Energy, family roles, language, mobility, mood, personality, self-care, social roles, thinking, upper extremity function, vision and work/productivity. Scores typically range from 49 (poor) to 245 (excellent). We defined good quality of life as at least 60% on the SSQOL scale as suggested in the study by Erban et al., [14] Finally, patients and their relatives were asked, if they would have given consent to surgery in retrospect, considering all events during initial stroke and subsequent recovery. The follow-up period ranged from at least 18 months to several years after surgery. All questionnaires were administered in a face-to-face interview and performed by the same examiner (Dr. F. Wang). All surviving patients completed the questionnaires on depression, SSQOL, and retrospective approval on surgical treatment by themselves or with the help of relatives. Continuous values are expressed as a mean ± SD (range), non-continuous values as median (range). Data were subsequently analyzed with the use of SPSS 13.0 for Windows package. Wilcoxon rank sum test and x2 were used for univariate comparisons as appropriate for continuous or categorical variables. A value of P < 0.05 was considered statistically significant. Results The study cohort comprised of 44 patients (34 men and 10 women), with a median age of 55.6 ± 9.4 years (range 34-74) and a median postsurgical follow-up period of 35.8 ± 17.3 months (range 18-81). The mean interval from symptom onset to surgery was 25.4 ± 41.2 h (range 1.5-250). The mean MAP was 133.5 ± 18.7 mmHg (range 96.7-170). The mean volume of ICH was 62.5 ± 28.5 cm 3 (range 30-150). Based on our own experience, the indication for operation on patients with hypertensive basal ganglia hemorrhage mainly relied on the level of consciousness preoperatively, rather than the volume of ICH. The median NIHSS and GCS score before surgical treatment was 19 (range 3-28) and 9 (range 6-15) respectively. At the time of the last follow-up, 13 patients had died (mortality rate 29.5%). The cause of death was uncal herniation as revealed by CT or cardio-pulmonal deterioration. Of the 31 patients who survived, 21 (67.7%) patients had a BI $ 60, 23 (74.2%) patients had a mRS < 4 and 21 (67.7%) patients had a SSQOL $ 60%, each representing a favorable outcome. There were no significant differences in the age, volume of ICH, and the time interval between onset of symptoms and surgery between patients in the death and survival groups whereas the mean MAP, median NIHSS, and GCS score were significantly different between the two groups [Table - 1]. Of the 31 surviving patients, 18 (58.1%) patients developed depression (BDI > 9). The predictors of depression included pre-operative NIHSS (high) and GCS (low) scores and postoperative BI (low), mRS (high) and SSQOL (low) scores [Table - 2]. In retrospect, 19 (61.3%) patients approved the surgery. Discussion World over there is a greater variability in the management of ICH. Spontaneous supratentorial ICH is associated with a very high immediate mortality, about 40%. [15] The mortality rate following surgical evacuation observed in our study was similar to the mortality rate reported in the retrospective study by Kanaya and Kuroda. [16] In their study, for hematomas more than 30 ml, surgical evacuation resulted in lower mortality compared to medical treatment (30% vs. 67%). In our study the mortality was related to pre-operative high MAP, high NIHSS score and low GCS score. In our opinion, control of blood pressure and careful selection of patients based on the preoperative NIHSS and GCS scores may help to reduce the mortality further. With the developments in neuroanesthesia, intensive care and surgical techniques, surgical treatment may be associated with reduced chances of dependency in patients with supratentorial ICH. [17] During the long-term follow-up period in this study, 21 (67.7%) patients with hypertensive basal ganglia hemorrhage had a BI $ 60, 23 (74.2%) a mRS < 4 and 21 (67.7%) a SSQOL $ 60% after operation, each representing a favorable outcome. In retrospect, 19 (61.3%) patients approved the surgery. Therefore, surgical treatment appears to be an option for selective patients with hypertensive basal ganglia hemorrhage. The reported frequency of post-stroke depression in previous studies ranged between 20% and 65%. [18] Depression is highly relevant for physical handicap and quality of life. [14] In our study, about two-thirds of patients who had surgery developed depression. The predictors of depression included preoperative NIHSS (high) and GCS (low) scores and postoperative BI (low), mRS (high) and low SSQOL (low) scores. Thus there is a need for long-term healthcare and treatment for depression in patients with hypertensive basal ganglia hemorrhage undergoing surgical evacuation. The limitations of our study include small sample size, patient selection bias, and no control group (only medical treatment). To avoid heterogeneity of data, future randomized surgical trials should carefully consider the quality of life associated with depression after surgery for patients with hypertensive ICH. In addition, the feasibility studies should be designed with sufficient statistical power to demonstrate a difference in depression rates between surgical intervention and conservative therapy. In conclusion, the current analysis shows that depression is a common long-term complication after surgical treatment. Both the NIHSS and GCS score before operation have critical roles to play in patient′s Quality of life associated with depression. References
Copyright 2010 - Neurology India The following images related to this document are available:Photo images[ni10015t2.jpg] [ni10015f1.jpg] [ni10015t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}