 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 58, No. 1, January-February, 2010, pp. 78-84 Original Article Can infusion tests be recommended for patients with giant hydrocephalus? Krzysztof Cieslicki, Ryszard Czepko1 Laboratory of Bioflows, Institute of Automatic Control and Robotics, Warsaw University of Technology and Correspondence Address: Krzysztof Cieslicki, Laboratory of Bioflows, Institute of Automatic Control and Robotics, Warsaw University of Technology, Poland, cieslick@mchtr.pw.edu.pl Date of Acceptance: 05-Jan-2010
Code Number: ni10016 DOI: 10.4103/0028-3886.60405 Abstract Background : The problem of adequate diagnosis of hydrocephalus
followed by administration of an effective treatment has not yet been
properly solved. Specifically, this pertains to the decision about the
surgical insertion of a flow diverting device. Keywords: Infusion test, intracranial compensatory parameters, normal pressure hydrocephalus Introduction The problem of adequate diagnosis of hydrocephalus followed by administration of an effective treatment have not yet been properly solved. [1] Specifically, this pertains to the decision about the surgical insertion of a flow diverting device (shunt), which bypasses the blocked pathways of the outflow of cerebrospinal fluid (CSF) from the intracranial space. The physical assumption for the effectiveness of such treatment is that the shunt will compensate the pathologically increased outflow resistance (Rout ). This establishes the physical basis for shunting and requires the measurement of Rout , which can currently be assessed only by challenging the CSF volume under invasive monitoring of intracranial pressure (ICP). One of the commonly used methods utilizes a constant rate of infusion which results in a slow upward trend in ICP toward a new steady state. At the simplest clinical approach, the difference between this state and the baseline pressures divided by the infusion rate yields the desired Rout value. [2],[3] Nevertheless, the interpretation of the infusion test (IT) is complicated by relatively long evolution time of the response toward the steady state and the increased presence of slow ICP fluctuations. A common way to increase the reliability of the Rout estimation is based on a computerized recording of the response followed by a least-squares optimization aiming to obtain the best value of Rout . [4],[5],[6],[7] Such approach is technically more complicated but promises viable estimates even if the plateau of the response has not been reached or is obliterated by slow wave fluctuations. A mathematical description of the ICP rise during infusion was first proposed by Marmarou et al.[8] and was further slightly modified by Avezaat et al. [9] Marmarou′s model has found application in qualifying the patient for hydrocephalic shunt implantation. [10] Excluding the cases with aqueductal stenosis, the clinical symptoms of giant hydrocephalus are similar to typical normal pressure hydrocephalus (NPH). So when Rout is increased, many of these cases seem to be good candidates for shunting. However, from the mechanical point of view, the real problem is the thin cerebral mantle, which can be a potentially dangerous factor in the case of postoperative overdrainage. Thus the question arises if possible changes in mechanical features of the brain are reflected by parameters characterizing compliance. As the dynamics of the ICP growth during infusion depends on intracranial compliance, the possible way to identify these parameters is the numerical identification of the infusion response function. The aim of this study is the examination of compensatory parameters of the intracranial space in giant hydrocephalus in contrast to the early and late outcome and analysis of the complications in shunted cases. They may throw some light on the problem-whether infusion test can be recommended in such cases. Materials and Methods From 153 patients admitted to the Neurosurgical Clinic of the Jagiellonian University in Krakow and examined for progressive symptoms suggesting NPH, we have chosen nine (five males and four females) patients with giant hydrocephalus. The choice was based on planimetric measurements of the ventricles, Evans ratio and ventricular index. Chosen patients had Evans ratio more than 0.5 (normal < 0.3), ventricular index more than 1.5 (norm. < 0.8) and third ventricular width more than 20 mm. Their ages ranged from 34 to 63 years with a mean of 49 years. None of the patients had expansive lesions, midline shifts of the ventricular system, ischemic changes or imagiological evidence to suggest impaired communication of the intracranial fluid spaces. The hydrocephalic signs were assessed according to the Sahuquillo and Rubio scale [11] and ranged from 5 to 14 (mean, 10 points). All the patients had undergone invasive testing to confirm the hydrodynamic component behind the preliminary diagnosis of hydrocephalus. In this case, lumbar infusion tests were performed using one puncture needle; the ICP response was measured with a piezoelectric transducer, sampled at 20 Hz and stored on a standard PC equipped with an analog-to-digital converter. In-house software [7] was used offline to fit the dynamic response, P(t), to the observed data using the following equation: [8],[9]
where P(t) is the adjusted response of ICP to an infusion starting at time t = 0; ICP B (mmHg) is is the measured baseline ("opening") ICP before the start of infusion; Q i is the given (2.0 ml/min) infusion rate of mock CSF; ICP e (mmHg) is the estimated asymptotic end-plateau value of ICP at infinitely long infusion time; E (ml-1 ) is the estimated elastance index of the cerebrospinal system; and P0 (mmHg) is the estimated offset parameter ("reference pressure") in compliance characteristics. The outflow resistance can be established from the above parameters as follows:
Conversely, the intracranial compliance can be calculated as a function of the ICP:
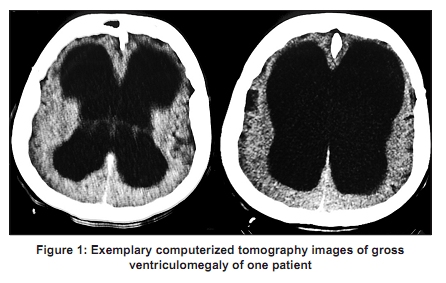
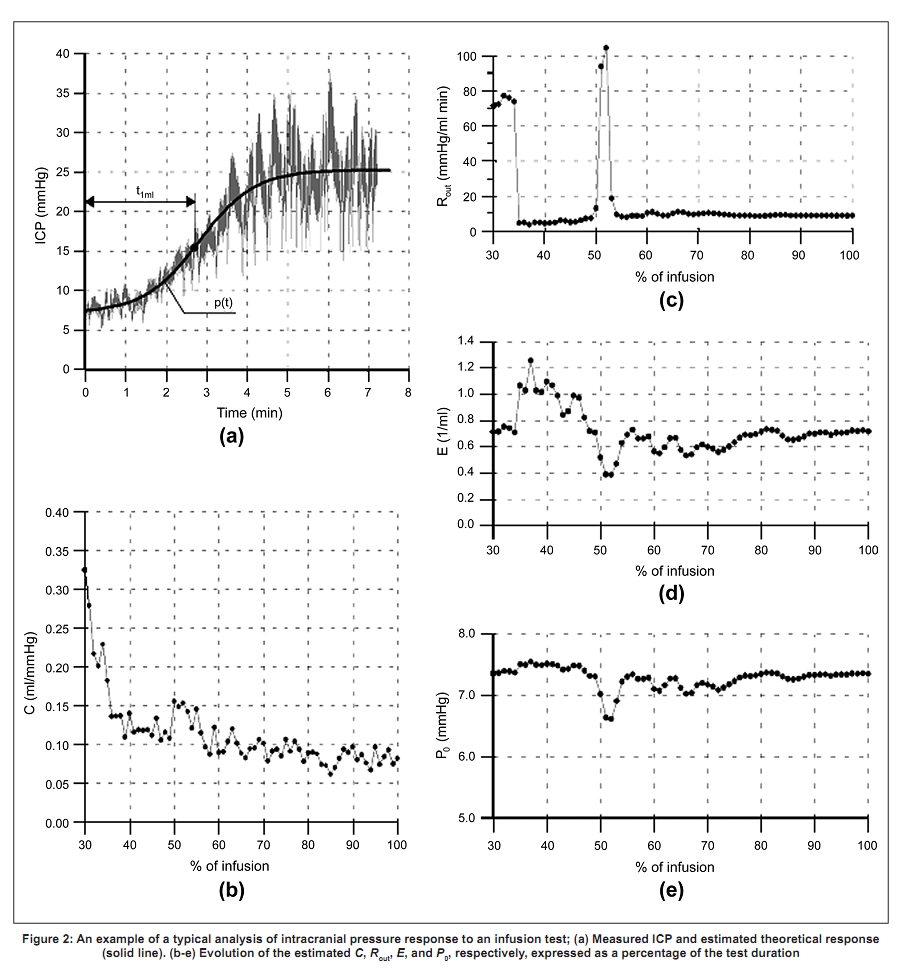
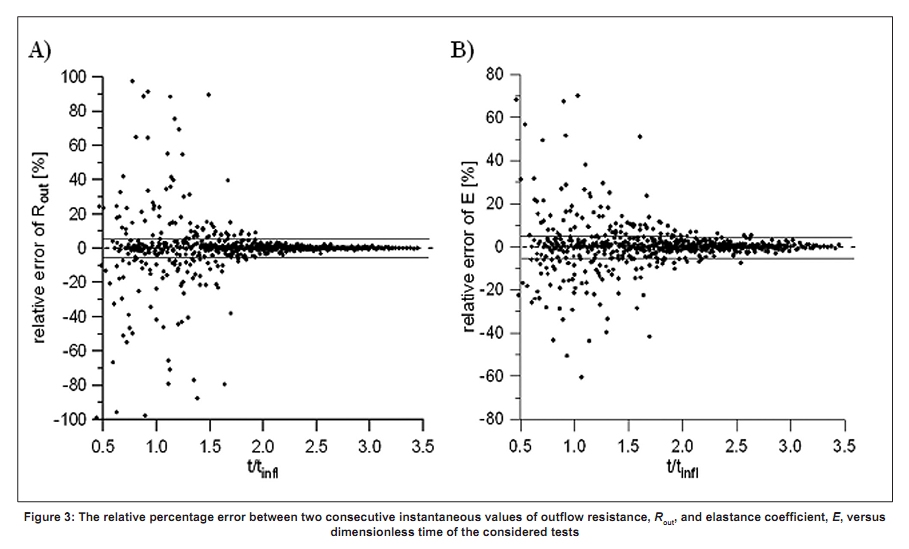
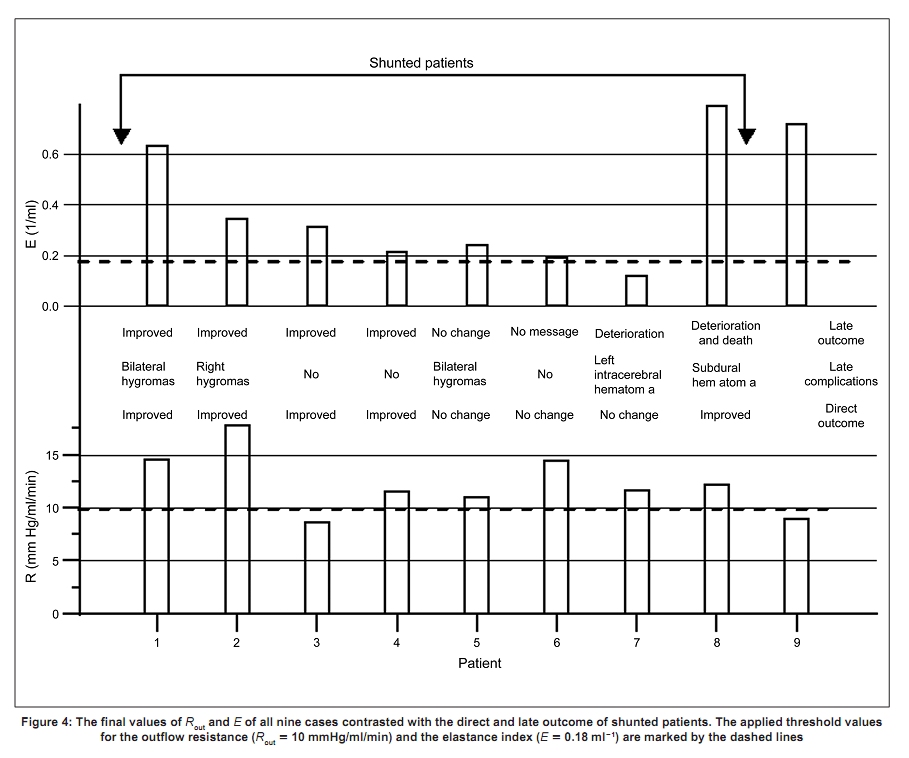
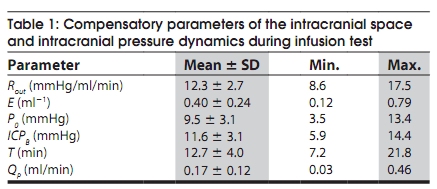
In the above equations, there are three parameters (ICPe , E, P0 ) that can all be fitted simultaneously by a nonlinear minimization algorithm. A value of the baseline pressure, ICPB , was determined from the period before the infusion commenced and was treated as a known constant. A correct identification of the Marmarou model parameters is made particularly difficult by the pulsatile, respiratory, and other waves of various origins that overlap with the test [12] and by numerous artifacts resulting from the patient′s movement. In order to find stable values of these parameters durin-g infusion, we have applied a computer-assisted method for their dynamic identifications. [7] The method depended on the repeated search for the best-fitting curve corresponding to the progress of the test. The evolution of parameters Rout , E, and P0 in time expressed as a fraction of the available ICP recordings was calculated and displayed together with the best-fitting curve, P(t), plotted online over the registered ICP. For quantitative estimation of the stability of identified parameters during infusion, the relative percent error, between their two consecutive, instantaneous values, was calculated. Of the nine patients, eight patients were shunted for the following indications: (1) clinical signs of hydrocephalus impairing the daily activity; (2) elevated value of the resistance to outflow over 10 mmHg/ml/min; and (3) positive CSF tap test with Rout below 10 mmHg/ ml/ min. In order to reduce the risk of postoperative overdrainage, the valve opening pressure was always at least 3-4 mmHg higher than the patient′s baseline CSF pressure, and each was armed with an anti-siphon device (ASD) or was originally equipped with a siphon control device (SCD). Medium pressure valves were implanted in five patients and programmable valves in further three patients. Programmable valves were set on 13-15 cm of H 2 O opening pressure. Patients were followed up for 9 months, the follow-up including clinical and computerized tomography (CT) assessment of the outcome. Results [Figure - 1] presents two CT images obtained for a single patient, characteristic for the analyzed group, with giant ventricles surrounded by a sliver of the brain. A slight margin of periventricular lucency around the frontal horns was visible. [Figure - 2] shows the results of the lumbar infusion test conducted for the same patient. The top graph on the left [Figure - 2]a displays the pressure-time recording with its final best-fit approximation, P(t), plotted over. The three graphs on the right [Figure - 2] c-e show the calculated evolution of parameters Rout , E, and P0 , respectively. The bottom graph on the left [Figure - 2]b displays the evolution of intracranial compliance, C, calculated from Eq. 3. As seen in [Figure - 2], the identified parameters changed significantly at the initial part of test without showing a clear trend. The resistance of the CSF outflow stabilized after reaching only 55% of the total infusion time. Intracranial compliance gradually diminished as the test progressed, showing remarkable fluctuations which reflected variations of ICP, E, and P0 . [Figure - 3] shows how identified parameters of CSF dynamics, Rout and E obtained for all the tests, stabilized during infusion. The inflection time of the best-fit test curve, tinfl [Figure - 2]a, calculated for each test was used to normalize the time of the relevant test. The inflection time corresponds to the moment from which the response, P(t), starts to flatten out. Results shown in [Figure - 3] clearly demonstrate that the correct identifications of the compensatory parameters were hardly possible unless the inflection time was reached. Stable values of Rout , E, and P0 always corresponded to the part of the P(t) curve above the inflection point. A test, should last at least two times longer than the inflection time, to determine the outflow resistance with an error of less than ±5%. To obtain the same error for the cerebral elastance index, the test should last longer, at least 2.5 x tinfl . In [Figure - 4], the final values of Rout and E of all patients are contrasted to the direct and late outcomes of shunted cases and the sources of developed complications. Mean final values, standard deviations, and the range of changes of all identified parameters of intracranial space compensation as well as additional features of IT dynamics, namely, the baseline pressure, time of infusion, T, and estimated CSF production rate, Q P, are set up in [Table - 1]. As can be seen, all patients had a normal value of the baseline pressure (not greater than 15 mmHg). Seven patients had Rout > 10 mmHg/ml/min, whereas the remaining two had Rout < 9 mmHg/ml/min. Nevertheless, the final decision of shunting was taken for eight patients, because one patient (number 3) with a low Rout value, 8.6 mm Hg/ml/min, was neurologically impaired and improved after the preoperative diversion test. One patient was not shunted due to a low Rout value, 8.9 mmHg/ml/min and also the patient had mild memory impairment and no other neurological signs of hydrocephalus. Only one patient (number 7) had a value of elastance index within the normal range (0.05 - 0.18 ml-1 ). [13] The remaining eight patients had their elastance index elevated above the upper limit. Five out of eight shunted patients significantly improved in a few days after surgery (62%), and three remained unchanged. During the nine months follow-up five (62%) patients developed complications: Subdural hygromas/hematomas in four and intracerebral haematoma in one. We had no information about one patient. One patient (number 8) died due to the huge subdural hematoma, two slightly deteriorated, and in the remaining patients the complications did not affect the outcome. In summary, definite improvement was noted during follow-up in four out of eight operated patients (50%). There was no correlation between post shunt improvement and any of the compensatory parameters but the study sample was too small to expect any significant association. Discussion Currently, the clinical importance of the results obtained by infusion test are extensively discussed in terms of predicting the shunt outcome, but their accuracy under time constraints of typical clinical settings is not addressed in a systematic way in the literature. From the present study, additionally supported by other results reported in a conference publication, [7] we may conclude that the test should last at least two and a half times longer than the inflection time to achieve ±5% accuracy. Despite a huge number of investigations [1],[2],[3],[4],[5],[6],[7],[10],[14],[15] so far, only the outflow resistance has gained significant evidence of prognostic value, however the abnormal pathological measures have not yet been defined. [16] In healthy volunteers Rout is not higher than 8 mmHg/ml/ min. [17] According to the literature, the highest normal value of Rout varies between 8 and 13 mmHg/ml/min. Generally, higher the Rout , measure, the greater is its prognostic significance and with a value above 17 mmHg/ml/ min, one can expect improvement in 95% of shunted patients. [16] In our series, the threshold of 10 mmHg/ml/ml was defined arbitrarily, and had an auxiliary rather than a prognostic value. We expected improvement after shunt based on unequivocal neurological signs corresponding with the radiological image. The clinical interpretation of cerebral elasticity is still a controversial issue. The elastance index is considered elevated (E > 0.18) for poor pressure-volume compensatory reserve. Almost all examined patients had the elastance index raised, sometimes considerably (max. 0.79) that would testify to the lack of intracranial space reserve in such patients with hydrocephalus. The physiological meaning of the reference pressure, P0 , is obscure and its range of change is not known. Most frequently, P0 is considered to be approximately equal to the sagittal sinus pressure. [19] With this assumption, we are able to estimate the individual rate of CSF secretion, Q P, in our patients, from the Davson formula:
[Table - 1] displays the mean value of CSF secretion as well as its standard deviations and the range of changes. The estimated mean (0.17 ml/min) was significantly lower than the typical production range given in the literature, [20] 0.27 - 0.45 ml/min. A reduced value of CSF secretion may endanger the health and life of shunted patients in the case of overdrainage. Time of regeneration of the lost fluid volume, which is inversely proportional to CSF secretion, is much longer than physiological. During that time the brain has a greater risk of collapse with all its consequences. In fact, our observations indicate a relatively higher risk of overdrainage in shunted patients with giant hydrocephalus, in spite of setting a medium (not low) value of valve opening pressures and ASDs or SCDs. The thin cerebral mantle is resistant to decompression, and can collapse producing subdural CSF collection or hematoma. Ventriculo-peritoneal (VP) shunt reduces ICP thereby increasing arterial transmural pressure which can promote bleeding. This could be the most probable cause of small intracerebral hematoma in one of our patient, because the other potential reasons of this complication, such as arterial hypertension, atherosclerosis of cerebral arteries, and hemostatic system disorders, were excluded. The maximal shunt flow according to the shunt specification may reach even 600 ml per 24 h (0.42 ml/min), as it was in this particular case that is 2.5 times more than the average CSF secretion rate. This study suggests that an increased value of the elastance index and a reduced value of CSF secretion seems to be a more characteristic feature for giant hydrocephalus than an increased value of outflow resistance (whereas eight patients had E $ 0.2 ml-1 , only three of them had Rout > 13 mmHg/ml/min, which is considered in the literature as pathologic). Occurrence of complication in patients with giant hydrocephalus with shunt implant makes the decision of shunting difficult. The risk of overdrainage in these cases is unacceptably high, despite the availability of many sophisticated shunting devices. Because of these observation we may suggest that the confirmed diagnosis of giant hydrocephalus is a relative contraindication to implantation, and also for IT, the results of which may be ambiguous. The above conclusion are further supported by the recent observation in the study by Masdeu et al. [21] They suggested that because of impaired physiological flow of the CSF in individuals with chronic giant hydrocephalus, these patients may develop alternative CSF pathways to preserve brain function. Such pathways indicate the biological adaptation to anomalous conditions and successful compensation and may be an alternative to the reduced CSF secretion that is reported by us. Acknowledgment The authors thank Mr. Richard Pyplacz for thorough language correction of the manuscript. References
Copyright 2010 - Neurology India The following images related to this document are available:Photo images[ni10016f4.jpg] [ni10016f3.jpg] [ni10016t1.jpg] [ni10016f2.jpg] [ni10016f1.jpg] |
| |||||||||





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}