 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 58, No. 1, January-February, 2010, pp. 85-89 Original Article The epidemiology and clinical management of craniocerebral injury caused by the Sichuan earthquake Lu Jia, Guo-ping Li, Chao You, Hao Li, Si-qing Huang, Chao-hua Yang, Hai Xiong, Yi-jun Zeng Department of Neurosurgery, West China Hospital of Sichuan University, 37 Guo Xue Xiang, Wu Hou District, Chengdu - 610 041, China Correspondence Address: Dr. Guo-ping Li, Department of Neurosurgery, West China Hospital of Sichuan University, 37 Guo Xue Xiang, Wu Hou District, Chengdu - 610 041, China, hxbslgp@163.com Date of Acceptance: 09-Oct-2009
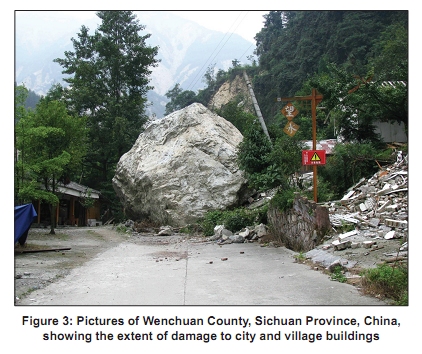
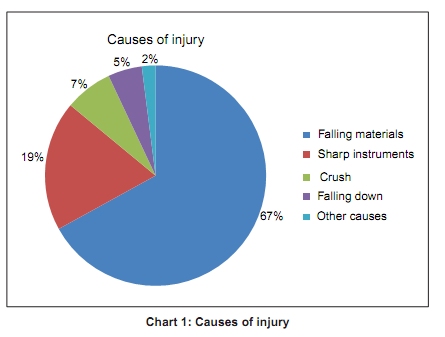
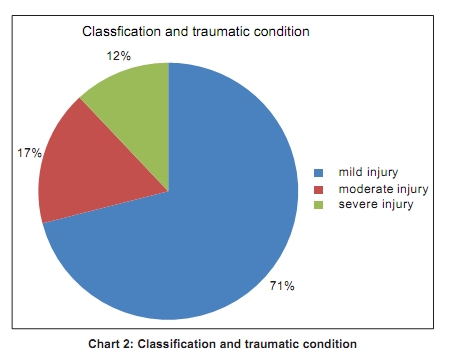
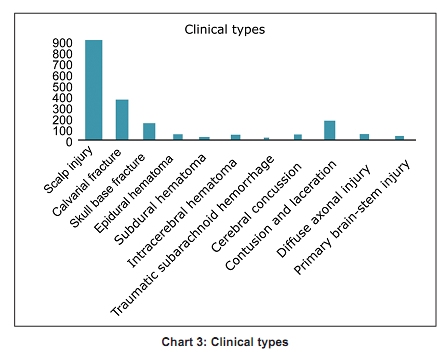
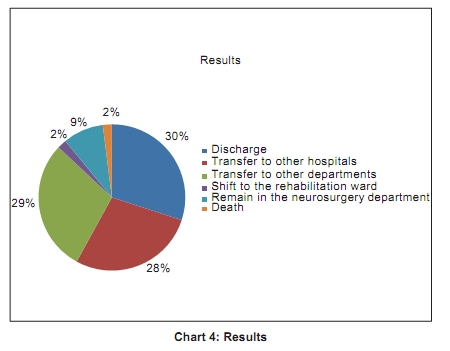
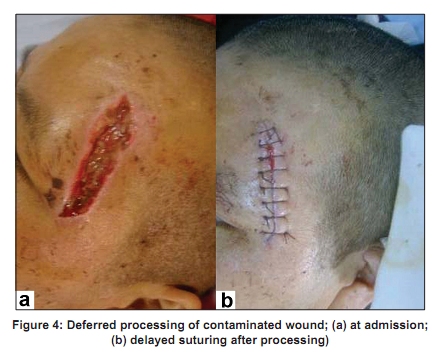
Code Number: ni10017 DOI: 10.4103/0028-3886.60406 Abstract Background : Earthquake is one of the most devastating natural disasters that threaten human lives. Worldwide more than 3 million deaths have been caused by earthquakes in recent 20 years. Keywords: Earthquake, head trauma, scalp infections, therapy Introduction Earthquake is one of the most devastating natural disasters that often threatens human lives. Worldwide more than three million deaths have been caused by earthquakes in the recent 20 years. [1] The Sichuan earthquake in China in June 2008, has resulted in approximately 70,000 deaths and more than 370,000 injuries. [2] The widespread effect of the quake destroyed a large number of cities and villages [Figure - 1],[Figure - 2],[Figure - 3]. It has been recorded as the deadliest earthquake in China since the 1976 Tangshan earthquake. [3] Adequate understanding of the clinical characteristics of craniocerebral injuries (CCI) caused by earthquakes and the experience gained in the diagnosis and treatment of the earthequake-related CCI is of critical importantance for optimal managing of the victims of major earthquakes and other disasters. In the 5.12 Sichuan earthquake, a total of 1,368 patients with earthquake-related CCI were admitted to the neurosurgery services of different hospitals located in Chengdu, Deyang, Mianyang and Guangyuan. This study reviews the clinical characteristics of the patients who sustained injuries in the earthquake. Clinical Data and Outcome Demography Following the earthquake 1368 (755 men and 613 women) patients with earthquake-related CCI were admitted to various hospitals in the region. The mean age of the patient population was 43.36 years (men: 25.9 years, women: 25.2 years, range: 1 month to 88 years). Source Of the 1368 patients included in the analysis, 701 were from three major hospitals in Chengdu, 233 from Mianyang, 201 from Deyang and 233 from Guangyuan. Causes of CCI The causes of injuries were: Falling building materials in 913 (67%) patients, sharp instruments in 256 (19%) patients, crush injury in 102 (7%) patients, and in 72 (5%) patients injuries were due to falls during escaping, while 25 (2%) patients were hurt by other causes [Chart - 1]. Classification of injury and state of the patients The type of injury was open cranial injury (OCI) in 657 (48%) patients and open CCI in 234 (17%) patients. Based on Glasgow coma scale (GCS) scoring system the injuries were classified as mild in 966 (71%) patients, moderate in 239 (17%) patients and severe in 163 (12%) patients. Cerebral herniation was observed in 42 (3%) patients [Chart - 2]. Clinical types Scalp injury was found in 891 (65%) patients, calvarial fracture in 382 (28%) patients, skull base fracture in 153 (11%) patients, intracranial hematoma in 140 (10%) patients (epidural haematomas: 56, subdural hematomas: 43, intracerebral hematomas: 41). In addition, 18 (1%) patients had traumatic subarachnoid hemorrhage; cerebral concussion in 53 (4%) patients, contusion and laceration in 155 (11%) patients, diffuse axonal injury in 47 (3%) patients and primary brain-stem injury in 25 (2%) patients [Chart - 3] . Time to treatment 248 patients (18%) received medical care on the first day of the earthquake; 479 (35%) on the second day; 401 (29%) on the third day and 240 (18%) on the fourth day or later. Treatment 704 patients received no treatment; 114 patients received emergent treatment and 12 patients had intubation. Of the 891 patients with scalp laceration, 316 received dressing and 36 received fixation. Time to admission 162 patients were admitted within 24 h after the earthquake; 215 patients within 24-48 h after the earthquake; 432 patients within 48-72 h and 559 patients were admitted on the fourth day or later. Concomitant injuries Bone fracture (286 cases in total) was the main concomitant injury, including limb fracture in 202 patients, spine fracture in 20 patients, pelvic fracture in 41 patients and rib fracture in 23 patients. There were 68 patients with thoracic injury, 32 patients with abdominal injury and 69 patients with crush injury. Maxillofacial trauma was found in 67 patients and shock occurred in 36 patients. Complications Wound infection of the head was noted in 118 (9%) patient; lung infection in 49 (3.5%) patients; post-traumatic seizures in 25 (2%) patients and acute renal failure in 29 (2%) patients. Therapeutic principles Treatment was administered to maintain vital signs and homeostasis as well as to prevent complications based on the ABC principles. Complete debridement and suturing were performed in the patients with open wounds within 72 h. For those with open wounds present for more than 72 h, bacteriological analysis was performed and debridement and suturing were done if the result of analysis was negative. Fractures were treated with the help of orthopedic surgeon. Antiepileptic treatment was given to those with seizures. Surgical debridement and operations to remove hematoma and necrotic tissues of the brain were performed in 98 patients with open injuries, intracranial hematoma and evident intracranial hypertension. Multidisciplinary therapy was administered in patients with combined injuries or multiple injuries. Thirty six patients with epidural hematoma and 31 with subdural hematoma underwent craniotomy. For patients with the most severe CCI, tracheal intubation was performed and venous passage was established in the emergency room. By June 12, 2008, 408 patients (30%) were discharged after recovery; 383 (28%) were transferred to other hospitals for further treatment; 394 (29%) were transferred to the department of orthopedics, department of burns and department of infectious diseases; 32 (2%) patients were shifted to the rehabilitation ward for rehabilitation training; 118 (9%) patiens remained in the neurosurgery department; and 33 (2%) patients died [Chart - 4]. Of the 58 patients with wound infection, 31 achieved primary healing or delayed primary healing [Figure - 4]. The Glasgow Outcome Scale (GOS) assessment of prognosis showed a score of 5 for 1121 patients (82%), 4 for 173 patients (13%), 3 or less for 74 patients (5%) among the 1368 patients discharged or transferred to other departments. Overall 33 patients died (2.41%). Discussion In the twentieth century, there were nearly 1,200,000 earthquake-related deaths worldwide, with 600,000 (50%) in China alone. Destructive earthquakes with a magnitude of more than 5 occurred in various provinces, autonomous regions and municipalities in China. In China, approximately 41% of the territory, 50% of the cites and 70% of the large and medium-sized cities with a population of more than 1 million are located in highly seismic zones with an intensity ≥7 on Richter scale. The Sichuan earthquake, which was the deadliest earthquake in China since the 1976 Tangshan earthquake, has resulted in approximately 70,000 deaths and injuries for more than 3,70,000 people. Up to 65% of earthquake-related deaths were related to craniocerebral and spinal injury. [4] The early mortality in the victims with CCI was as high as 30%. [5] Thus, an adequate understanding of the clinical characteristics of the earthquake-related CCI and also the knowledge and experience thus gained in the diagnosis and treatment of earthquake-related CCI will be of great importance and of use in managing victims of earthquake and other disasters. In the previous studies, earthquake-related injuries were mainly skeletal injuries followed by cranial injuries, about 15 - 40% of the total injuries. [1],[4],[5] In the Sichuan earthquake, CCIs accounted for 11% of the earthquake-related injuries in different hospitals. This figure was much lower than the reported frequency in the literature. Of the CCIs, mild to moderate injuries accounted for 85% and severe injuries accounted for 15%. However, in the previous studies, earthquake-related severe CCIs accounted for approximately 30% of all CCIs. Probably this lower frequency may be related to the fact that majority of patients with severe CCI might have died before reaching the hospitals. In addition, the 5.12 Sichuan disaster was a shallow-focus earthquake, which had seriously and directly affected an area of about 100,000 Km 2 . The vast area within 200 km of the epicenter was directly affected and numerous towns had been terribly destroyed. Means of transportation and communication, water and electricity supply, and medical facilities were also ravaged. Continuous aftershocks had also contributed greatly to the difficulties in the rescuing operations. In some heavily affected areas, the medical system was almost paralyzed, thus nictitating external medical assistance. In some other affected areas, although the buildings were not totally destroyed, water and electricity supply were suspended, and the hospitals only acted as transfer stations for first aid because the medical facilities did not function optimally. Under these circumstances, there was a greater chance of survival for patients with mild to moderate CCI only while, the majority of patients with CCI were not able to receive immediate treatment due to delayed excavation, transferring and rescuing. After the main shock, most of the patients were transferred to the hospitals between Day 3 and Day 4. Patients with severe CCI might have great difficulties to have adequate and effective treatment in time for all the attended complications of severe CCI, while patients with mild to moderate CCI had fair chances of adequate treatment. This had a reflection in our study, the proportion of patients with CCI treated was very small. For the reasons above, there is an urgent need for improving early field first aid and also subsequent appropriate treatments in disaster medicine to bring down the death rate of the patients with severe CCI. In this report in 67% of the patients the CCI was related to the falling building materials thus suggesting that the major causative factor for CCI during earthquake is collapse of buildings. In this study the characteristics of earthquake-related CCIs in the treated were either open cranial injury (48%) or open CCI. (17%). In the treated patients who had open cerebral injury or CCI, 35% did not undergo debridement and suturing and 23% developed infection due to nonstandard or incomplete debridement. Patients were classified and treated appropriately according to wound status on admission. At the time of admission, 23 patients with wounds were not bandaged for more than five days. In these patients, 17 patients who had a negative smear test achieved primary healing after complete debridement and suturing. For those with a nonbandaged wound and with signs of infection at the time of admission, secretions were collected for analysis and dressing change was done daily to promote healing. For those with bacterial infection, pus was collected immediately for analysis and the original suture was removed to facilitate open drainage. Various foreign bodies such as hair, bone fragments, mudstones and leaves were found in 16 patients. Following removal of the foreign bodies, secretions were analyzed. The wound healing was achieved due to daily dressing change. Cerebrospinal fluid leakage, wound infection, skin defect and skin flap necrosis were present in seven patients with open CCI, which made the later treatments more difficult. This suggests that the complexity of traumatic condition was associated with serious contamination and that early debridement had been performed under circumstances when there was a lack of professionals, surgical equipment or standard and effective therapeutic methods. Therefore, early, effective and standard treatments are important for earthquake-related patients. Associated medical conditions including shock, limb fractures, crush injuries and multiple organ failure such as acute renal impairment were present in the majority of 163 patients with severe CCI. Multidisciplinary treatment regimens based on the ABC principles were instituted in these patients. Twenty-seven patients with severe CCI and associated medical complication needing craniocerebral surgery had appropriate treatment for the medical conditions before the operation. Of these 27 patients, 23 patients had successful postoperative recovery and four patients died of severe shock. Twenty-nine patients who had associated acute kidney injury had hemodialysis after craniocerebral operation, 17 patients had good recovery and 12 died of renal failure and refractory cerebral edema and hernia. Of the 13 patients with associated limb fracture, 3 patients had compartment syndrome and decompressive surgery was performed by neurosurgeon and orthopedic surgeons. Distal limb function could be preserved in all the 3 patients. There were 17 deaths caused by late cerebral hernia. Of the 163 patients with severe CCI, 33 (20%) patients died. This relative low mortality was probably related to the effective multidisciplinary treatment. The main types of earthquake-related CCI include injuries by falling objects, multiple injuries with a mild to moderate severity and scalp injuries. Early complete debridement of the wound may minimize the risk of infection. For seriously injured patients, a multidisciplinary treatment should be adopted to save the life. Early neurosurgical management plays an important role in improving the survival rates. Development of effective treatment strategies for severely injured patients is a subject for a well designed investigation. References
Copyright 2010 - Neurology India The following images related to this document are available:Photo images[ni10017f3.jpg] [ni10017f4.jpg] [ni10017c3.jpg] [ni10017c4.jpg] [ni10017f1.jpg] [ni10017f2.jpg] [ni10017c2.jpg] [ni10017c1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}