 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 58, No. 1, January-February, 2010, pp. 95-98 Brief Report Spectrum of emergency department presentation in patients of acute intermittent porphyria: Experience from a North Indian tertiary care center Susheel Kumar, Navneet Sharma, Manish Modi 1 , Aman Sharma, Sushil Mahi, Subhash Varma Departments of Internal Medicine, 1 Neurology, Postgraduate Institute of Medical Education and Research, Chandigarh - 160 012, India Correspondence Address: Dr. Susheel Kumar, Department of Internal Medicine, Postgraduate Institute of Medical Education and Research, Chandigarh - 160 012, India, sk_bhutungru1977@yahoo.co.in Date of Acceptance: 05-Jan-2010
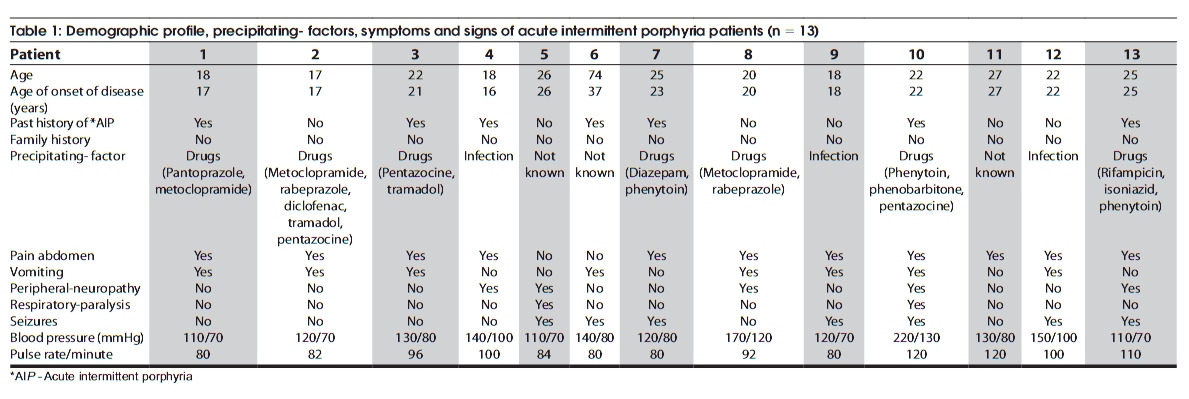
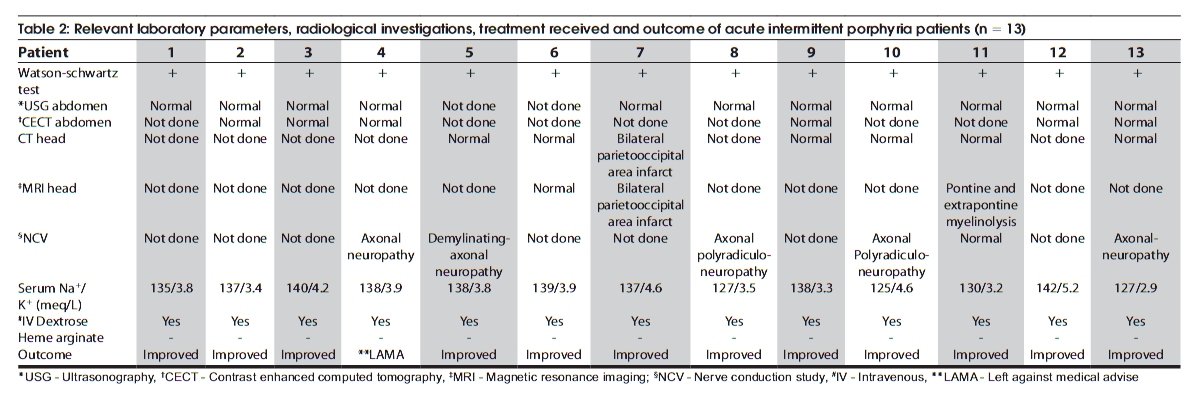
Code Number: ni10019 DOI: 10.4103/0028-3886.60410 Abstract Of the porphyrias, acute intermittent porphyria (AIP) is the most frequently encountered porphyria. The clinical characterestics of thirteen patients of AIP who presented to the Emergency Department were analyzed. The most common precipitating factor was drugs. Eleven patients presented with pain abdomen. Neurological manifestations included: Seizures in six and motor weakness in six. Of the four patients with hyponatremia, three had associated neuropathy and the fourth patient demonstrated a severe course marked by pontine-extrapontine myelinolysis and profound adrenergic activity. In conclusion, even though AIP is less frequently reported from India the emergency physicians should be vigilant to exclude the diagnostic possibility of AIP in a patient with an appropriate clinical setting.Keywords: Acute intermittent porphyria, emergency presentation, hyponatremia Introduction Porphyrias are a group of metabolic disorders associated with generation of excess of porphyrin intermediates or their precursors and acute intermittent porphyria (AIP) is the most frequently encountered porphyria. [1],[2],[3],[4] This study analyzed the presenting features, hospital course, complications and outcome in patients with AIP presenting to the Emergency Department (ED) of a tertiary care hospital. Materials and Methods This study was carried out at the Postgraduate Institute of Medical Education and Research, Chandigarh. Clinical records of all the patients with AIP presented to the ED from January 1996 to March 2008 were reviewed and relevant clinical details were noted in a predesigned instrument. Diagnosis of AIP was based on the characteristic clinical history including pain abdomen, autonomic dysfunction, neuropsychiatric manifestations and urine porphobilinogen (PBG) positivity. [5] Demographic profile, family history, history of previous acute attacks, possible precipitating factors, presenting symptoms and physical findings were recorded. Details of medications responsible for precipitating the acute attacks were noted. Laboratory data included urine PBG test, serum electrolytes, renal and liver function tests. Urine PBG detection was done by Watson-Schwartz test. Findings of the imaging modalities including ultrasonography, contrast enhanced computed tomography (CECT) and magnetic resonance imaging (MRI) were noted. Complications developed during hospital stay and ultimate outcome was also noted. Results During the study period 13 patients (eight male and five female) with AIP presented to ED [Table - 1] and [Table - 2]. Mean age at the time of presentation was 25.7 ± 14.9 years. Six patients presented with acute attack for the first time while the remaining seven patients had previous history of acute attacks. Most common precipitating factor was drugs (seven patients) [Table - 1]. Eleven patients presented with pain abdomen. Three patients had history of passing red-colored urine. Four patients had hypertension at the time of presentation and two of them went on to develop chronic hypertension requiring long-term antihypertensive medications. Six patients had acute seizures during the present attack and one patient had history of seizure eight years back. Seizure type was generalized tonic-clonic seizure (GTCS) in six patients and focal onset tonic-clonic seizure with secondary generalization in one. Five patients were taking gabapentin while two patients were on clonazepam. Seven patients had weakness, five patients had weakness in the form of acute flaccid quadriplegia and two patients had quadriparesis. Electrodiagnostic studies showed evidence of axonal neuropathy in one, axonal polyradiculoneuropathy in three and mixed axonal and demyelinating neuropathy in one. MRI in one patient showed features suggestive of pontine and extrapontine myelinolysis while another patient had acute non-hemorrahgic infarcts in bilateral occipital and parietal areas. Of the four patients with hyponatremia, three were complicated by neuropathy whereas the fourth patient demonstrated a severe course marked by pontine-extrapontine myelinolysis and profound adrenergic activity. One patient with hyponatremia had features of hypertensive emergency. Length of hospital stay ranged from two to 75 days. High- dose dextrose was given to all the patients. Due to the non-availability, heme arginate could not be given. Of the thirteen patients, twelve patients had improvement in their respective symptoms at the time of discharge. Discussion In this series acute attacks of AIP in the majority occurred after puberty and the predominant triggering factor was drugs followed by infections similar to the observations in the earlier series. [3],[4],[6] In patients with AIP the most common presenting complaint is abdominal pain. [1],[2],[3],[4] Hypertension as a manifestation of autonomic dysfunction is commonly seen during the acute attacks [1],[2],[3],[4],[7],8] and at times the presentation can be a hypertensive emergency. [5],[9],[10] In this series, four patients had hypertension at the time of presentation and one of them was in hypertensive crisis. Hyponatremia has been found to be a marker of severe attack. [5] In this series patient with hyponatremia had more severe disease manifestations. Seizures either focal or generalized occur in 3-15% of patients with AIP. [11],[12] In a study of 268 patients with AIP, seizures occurred in ten (3.7%) patients. [12] The treatment of seizures complicating porphyria is especially difficult because many common antiepileptic drugs are contraindicated in porphyria. Benzodiazepines, especially clonazepam may be beneficial during acute attacks. Gabapentin, vigabratin and leviteracetam have also been found to be safe for the treatment of seizures in patients with AIP. [13],[14],[15],[16],[17] Weakness during acute attack of AIP has been reported in 42-68% of patients. [2] Seven patients (53.8%) had presented with either acute quadriparesis or quadriplegia in our study. Nerve conduction study revealed neuropathy in five patients. In a study, 57% of patients of AIP demonstrated neuropathy but only three patients developed quadriparesis. [5] Conclusion Our study suggests that AIP related emergencies even though rare in India, can present to the ED and the diagnostic possibility of AIP should always be considered in patients with appropriate clinical setting. AIP related emergencies are potentially treatable. References
Copyright 2010 - Neurology India The following images related to this document are available:Photo images[ni10019t2.jpg] [ni10019t1.jpg] |
| |||||||||

{kind=link}
{kind=link}