 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 58, No. 1, January-February, 2010, pp. 103-105 Brief Report Recovery of oculomotor nerve palsy following surgical clipping of posterior communicating artery aneurysms Vamsi K. Yerramneni, P. Sarat Chandra, Manish K. Kasliwal, Sumit Sinha, Ashish Suri, Aditya Gupta, Bhawani S. Sharma Department of Neurosurgery, All India Institute of Medical Sciences, New Delhi - 110 029, India Correspondence Address: Dr. P Sarat Chandra, Department of Neurosurgery, Neuro Sciences Centre, All India Institute of Medical Sciences, Ansari Nagar, New Delhi - 110 029, India, saratpchandra@gmail.com Date of Acceptance: 07-Oct-2009
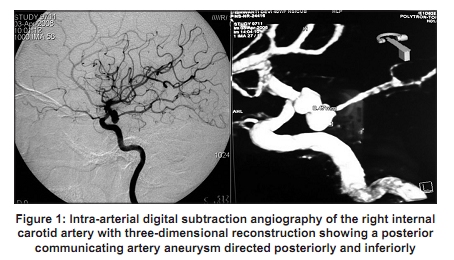
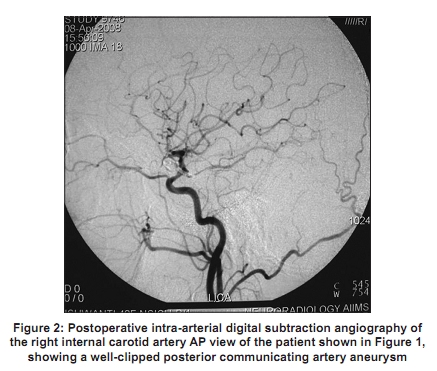
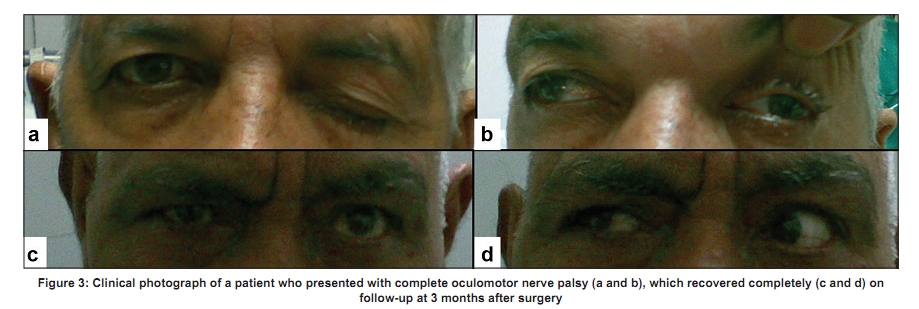
Code Number: ni10021 DOI: 10.4103/0028-3886.60413 Abstract Oculomotor nerve palsy (ONP) can be the presenting feature of ruptured or an unruptured posterior communicating artery (PcomA) aneurysm. Etiopathogenesis and recovery of ONP following treatment of PcomA aneurysm has been a subject of controversy. Case records of thirteen patients (mean age 42 years (range 19-65 years), M:F: 3:10) with PcomA aneurysm and ONP who underwent surgery over a period of eight years were analyzed. Twelve patients presented with subarchnoid hemorrhage and one had unruptured aneurysm. The interval between the onset of symptoms and surgery ranged between 4 and 70 days (mean 16.7 days). All the four patients with partial ONP had complete recovery and of the nine patients with complete ONP, six had complete recovery and three had partial recovery. The recovery of the ONP is influenced by the degree of preoperative deficit. Although clipping of the aneurysm probably expedites the recovery of the third nerve palsy, age, sex and timing of surgery may not have any influence on the recovery patterns.Keywords: Aneurysm, oculomotor palsy, outcome, posterior communicating, recovery, surgery Introduction Oculomotor nerve palsy (ONP) is often the presenting clinical feature of ruptured or unruptured aneurysm of posterior communicating artery (PComA). [1],[2],[3] Compression of the oculomotor nerve by the aneurysmal sac or hemorrhage associated with rupture is considered the plausible mechanism of the ONP. [1] Aneurysms facing posteriorly, inferiorly and laterally extending under the tentorium have been particularly implicated to cause third nerve palsy. Surgery by decompression of the aneurysm sac is associated with improvement of the ONP. [4],[5] Earlier studies have analyzed the factors associated with recovery of ONP after microsurgical clipping and coiling. [6],[7],[8] We analyzed our experience of recovery patterns of ONP in patients with PComA aneurysms. Materials and Methods Seventy-two patients with PcomA aneurysm were treated at our institution between 2001 and 2008. Thirteen patients who presented with ONP formed the study group [Figure - 1]. All patients underwent microsurgical clipping of the aneurysm. The case records of these patients were reviewed till the last follow-up. Complete ONP was defined as presence of diplopia, ptosis, complete ophthalmoplegia and pupillary abnormality. Partial preoperative ONP was identified as similar symptoms associated with partial extraocular movement in upward, medial, and downward gazes and/or pupillary sparing. Complete recovery of ONP was defined when the patient reported no diplopia or photophobia in any gaze, complete resolution of the ptosis, full range of ocular movements in all the directions, and normal pupil reaction. Time to ONP recovery was calculated from the day of clipping till the recovery of extraocular movements. Surgical procedure All the patients underwent pterional craniotomy and clipping of the aneurysm. Following clipping, the aneurysm sac was punctured, blood and clots were removed and the sac was decompressed. The sac was then dissected away from the nerve without handling the third nerve. Blood clots, if present, were washed from the cisternal spaces and papaverine was instilled in the cisternal space at the end of the surgical procedure. Follow-up Patients were followed-up at seven days, three months, six months, one year and then annually thereafter. All patients underwent postoperative angiography to confirm complete clipping of aneurysm, as judged by the treating neurosurgeon and neuroradiologist [Figure - 2]. Statistical analysis was performed using SPSS software version 15. Differences were considered significant at the level of P < 0.05.The influence of age, sex and timing from ictus to surgery on the recovery pattern was analyzed using the Mann-Whitney and x2 tests. Result The study patient population, thirteen patients with ONP, accounted for 19% of all the patients with PcomA aneurysm operated during the study period. There were ten females and the age ranged between 19 to 65 years (mean 42 years). Of the thirteen patients, one patient presented with unruptured PcomA aneurysm and twelve patients with subarchnoid hemorrhage (SAH). SAH grade (Hunt and Hess) was I, II, III and IV in two, six, three and one patients respectively. In patients with SAH, the duration between ictus and clipping ranged from 4 to 70 days (mean 16.7). All the three patients with partial preoperative ONP had complete recovery. Of the nine patients with complete preoperative ONP, six had complete recovery and three had incomplete recovery [Figure - 3]. Of the nine patients with complete ONP, two patients who presented on day 30 and day 40 of ictus had partial recovery of ONP at the time of presentation and both of them had complete recovery of ONP after surgery. The patient who presented on day 70 of ictus had partial recovery of ONP at the time of presentation and the recovery remained partial even after surgery. The mean follow-up was 17.5 months. (range, 3-25 months). Ocular movements recoved first followed by the pupillary reaction and ptosis. In some patients, there was a significant improvement in all the components of the third nerve palsy within a week after surgery. All the patients who had complete improvement had it so by their first follow-up visit at 3 months postoperatively. In all these patients, the aneurysm was directed inferiorly and posterolaterally, except for one patient who had a superiorly and posterolaterally directed aneurysm. There was no significant effect of age, sex or timing of surgery from ictus on the postoperative recovery of the ONP. Kappa statistics (measure of agreement) were used for analysis. Although statistically it was not significant (P = 0.19), the observations suggest that the status of preoperative third nerve palsy determines the postoperative recovery. Discussion Of the causes of ONP, intracranial aneurysms accounts for approximately 13.8%. [3],[5] Isolated ONP can be presenting feature of ruptured PcomA aneurysm and the reported frequency of third nerve palsy varies from 34 to 56%. [3],[5] Impairment of oculomotor nerve function has been attributed to the direct compressive effect of the enlarging aneurysmal sac or to the irritating effect of the adhesions and to the subarachnoid blood in case of ruptured aneurysms. [1] Painful ONP may be a warning sign and may indicate an impending aneurysmal rupture. [9] Third nerve palsy caused by the aneurysm can be complete in approximately 46% of the patients within 24 h of ictus and by one week, 66% experience complete palsy. [3] Although classically pupil is involved, it can be spared with the compressive lesion involving the inferior portion of the nerve. [10] Early surgery in patients with Pcom A and ONP is associated with possible complete recovery of ONP. [5],[11] Late surgery, 10-14 days after onset of complete palsy has been reported to be associated with less chances of complete recovery. [1],[3] One of our patients with complete ONP who had operation 70 days of ictus had poor recovery. Persistent aneurysmal sac compression resulting in extensive damage may be the cause for precluding complete recovery even after surgery.In our study the lack of significant association between timing of surgery and recovery may be due to small number of patients. In some patients with complete ONP early surgery may not result in complete recovery. [1] Two of our patients had partial recovery in spite of having early surgery within 10 days of ictus. This may probably be related to the individual susceptibility of the oculomotor nerve to transient compression. Kyriakides et al., [4] in their review, suggested that the preoperative severity of ONP determines the chance of postoperative recovery. Similar were the findings in our study. There seems to be a pattern in the recovery of third nerve palsy in patients with Pcom A treated surgically: Ptosis is the first sign to recover with the recovery generally starting in the first month postoperatively and full recovery taking several months. [1],[3],[4],[11] Although the resolution of ptosis is usually complete, extraocular muscle function frequently remains impaired, probably as a result of aberrant regeneration. [3] The results of comparative studies in the recovery pattern of ONP between patients with clipping and patients with coiling was quite variable. [4],[6],[8] The fact that coiling does not relieve the mass effect caused by the aneurysmal sac has raised concerns regarding the outcomes of third nerve palsy. In their retrospective study Chen et al., had observed no differences in the recovery patterns of third nerve palsy between patients having coiling and patients having clipping. In their study the timing of the procedure had also no bearing on the recovery pattern. [7] Our study suggests that the severity of preoperative ONP is probably the most important factor determining the pattern of recovery of the third nerve palsy associated with posterior communicating artery aneurysms. Clipping of the aneurysm probably expedites the recovery of the third nerve palsy. However the time interval between the ictus and operation may not have any bearing on the recovery pattern. References
Copyright 2010 - Neurology India The following images related to this document are available:Photo images[ni10021f2.jpg] [ni10021f1.jpg] [ni10021f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}