 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
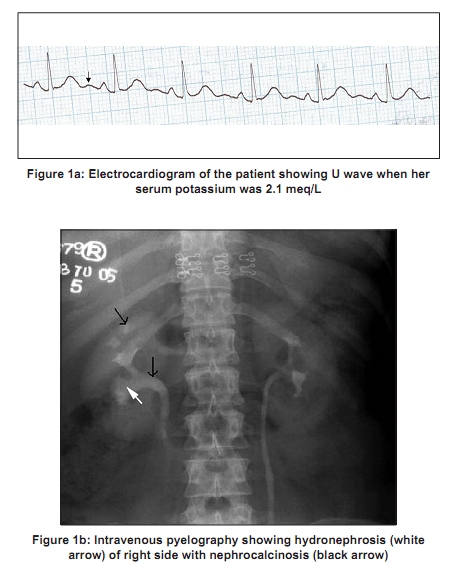
Neurology India, Vol. 58, No. 1, January-February, 2010, pp. 106-108 Case Report Renal tubular acidosis presenting as respiratory paralysis: Report of a case and review of literature J. Kalita, P. P. Nair, G. Kumar, U. K. Misra Department of Neurology, Sanjay Gandhi PGIMS, Lucknow, India Correspondence Address: Dr. J Kalita, Department of Neurology, Sanjay Gandhi Post Graduate Institute of Medical Sciences, Raebareily Road, Lucknow - 226 014, India, jkalita@sgpgi.ac.in Date of Acceptance: 02-Jul-2009
Code Number: ni10022 DOI: 10.4103/0028-3886.60415 Abstract Respiratory paralysis due to renal tubular acidosis (RTA) is rare. We report a 22-year-old lady who developed severe bulbar, respiratory and limb paralysis following respiratory infection. She had hypokalemia (1.6 meq/L) and hyperchloremic (110 meq/l) acidosis (pH 7.1). She was diagnosed as distal RTA by ammonium chloride test. She improved following sodium bicarbonate and potassium supplementation. RTA should be differentiated from familial periodic paralysis (FPP) because acetazolamide used in FPP aggravates RTA and sodium bicarbonate used in RTA aggravates hypokalemic periodic paralysis.Keywords: Hypokalemia, paralysis, renal tubular acidosis, respiratory paralysis Introduction Familial periodic paralysis (FPP) and renal tubular acidosis (RTA) have similar clinical picture with rarity of facial, ocular, bulbar and respiratory muscle weakness [1] although both these conditions are due to different pathophysiological mechanisms. In FPP, there is redistribution of K+ across the cell membrane, which is attributed to mutation in two genes encoding subunits of voltage-gated calcium or sodium channel (CACNA1S and SCN4A) of skeletal muscles. [2] In RTA on the other hand, there is loss of K+ due to impaired handling of K+ in the renal tubules resulting in impairment of acidification of urine. Excretion of other ions such as Na+ and Ca++ increases bicarbonate loss. [3] Respiratory involvement and severe paralysis is regarded to be rare in RTA and only 15 patients in English literature could be found. [1],[4],[5],[6],[7],[8],[9],[10],[11],[12],[13],[14],[15],[16] It is important to differentiate RTA from FPP because the principles of management and prophylaxis are different. We report a rare case of RTA who had respiratory paralysis and review the relevant literature. Case Report A 22-year-old postgraduate female student noted proximal muscle weakness in the morning and had difficulty in getting up from squatting position. The weakness progressed over a few hours and she experienced difficulty in turning in bed, swallowing and speaking. On the third day she developed breathing difficulty, drowsiness and carpopedal spasm. She had suffered from fever and cough five days prior to this illness which had lasted for two days. On examination patient was drowsy, dyspnoeic and was unable to move, swallow or speak. Her blood pressure was 150/50 mm Hg, pulse 96/min irregular, respiratory rate 40/min and responded to command by eye movement and closure. She had flaccid quadriplegia of Grade 0. Biceps, triceps, knee and ankle reflexes were absent. She was intubated and ventilated. Chvostek and Trousseau signs were present. Her hemoglobin was 8.9 g/dl, leucocyte count 16400/mm 3 , erythrocyte sedimentation rate 31 mm for the first hour, fasting blood sugar 70 mg/ dl, BUN 12 mg/dl, serum creatinine 0.9 mg/dl, uric acid 3.2 mg/dl, AST 880 IU/L, ALT 43 IU/L, creatine kinase 190 IU/L, bilirubin 0.6 mg/dl, calcium 6.9 mg/dl, phosphorous 1.9 mg/dl and potassium was 1.6 meq/l. Blood gas analysis revealed pH 7.1 (N = 7.35-7.45), serum potassium 2.1 (N = 3.5-4.5) mEq/L, serum sodium 136 (N = 135-148) mEq/L, PCO 2 52 (35-45) mmHg, PO 2 130 (80-100) mmHg, HCO 3 16.5 meq/L, chloride 110 mEq/L and an anion gap of 10 suggesting hyperchloremic normal anion gap metabolic acidosis. Electrocardiogram showed multiple premature ventricular ectopics and U waves [Figure - 1]a. She was treated with intravenous sodium bicarbonate 20 mEq, and KCl 20 mEq over 2 h following which her cardiac rhythm normalized. After administration of 160 mEq of potassium over the next 10 h of hospitalization, her muscle power and respiration improved and she was extubated. Her serum potassium at that point was 3.1 mEq/L. Within 48 h her blood pH and serum potassium were normalized. Ammonium chloride test was later carried out by administering 0.1 mg/kg ammonium chloride orally after obtaining blood pH, bicarbonate and urinary pH. These parameters were measured hourly for 6 h and revealed lack of acidification of urine (pH = 8) in spite of increasing acidosis of blood from 7.42 to 7.29 suggesting distal RTA. Her 24-h urinary protein was 280 mg, serum vitamin D level was 21.86 (normal 9-47) ng/ml and serum parathormone level 393.3 (normal 9-55) pg/ml. Urine and blood cultures were sterile. Radiographs of chest and pelvis were normal but plain radiograph abdomen revealed bilateral renal calculi. Ultrasonography of abdomen revealed cholelithiasis and intravenous pyelography bilateral hydronephrosis [Figure - 1]b. The patient was prescribed uriliser (potassium citrate and ammonium citrate) 10 ml thrice daily, calcium carbonate 500 mg thrice daily and vitamin D 1 mcg daily. She has been asymptomatic for the last three years on these treatments. Discussion Our patient suffered from severe hypokalemia resulting in bulbar, respiratory and limb weakness due to distal RTA. The diagnosis of distal RTA was based on hyperchloremic metabolic acidosis and positive ammonium chloride test in which increasing acidemia did not result in acidification of urine and urine pH remained higher than 5.5. In RTA acidosis and hypokalemia can be life-threatening during stress or an intercurrent illness as in our patient. Severe hypokalemia was associated with cardiac arrhythmia and respiratory paralysis resulting in medical emergency necessitating artificial ventilation. Only 16 patients including our patient of hypokalemia due to RTA have been associated with respiratory paralysis. [1],[4],[5],[6],[7],[8],[9],[10],[11],[12],[13],[14],[15],[16] Their age ranged between five and 55 years and all but two were females. Potassium level in these patients has ranged between 0.8 mEq/L to 2.09 mEq/L. The precipitating factors included diarrhea in 12, glue sniffing and alcohol in one patient each. In our patient also the acute attack of paralysis was triggered by infection. The associated systemic illnesses were Sjogren syndrome in five, [4],[5],[6],[7],[8] chronic active hepatitis in two, [9],[10] interstitial nephritis in two [7],[10] and diabetes insipidus in one. [6] Only one of these studies did the ammonium chloride test for confirmation of distal RTA. [5] Muscle weakness in RTA is common but respiratory paralysis is rare and is a serious complication. The progression to respiratory paralysis may be influenced by individual susceptibility and sensitivity towards hypokalemia and probably also transmembrane potassium gradient of respiratory muscles. The majority of reported patients with RTA with respiratory paralysis were females. With respiratory support and correction of metabolic abnormality all the patients had a good outcome. Patients with RTA with respiratory failure and ventricular fibrillation have been reported from Thailand. This condition occurs in otherwise healthy adults and sometimes resulted in nocturnal death. [17] Type I RTA may be familial and autosomal dominant is the commonest of inheritance. X-linked, autosomal recessive, and sporadic form has also been reported. In our patient there was no family history. Mutation in chloride bicarbonate exchanger gene has been found in the autosomal dominant form. Other diseases associated with RTA Type I are galactosemia, Ehler Danlos′s syndrome, Fabry′s disease, Wilson′s disease, hereditary elliptocytosis, Sjogren′s syndrome, hypogamaglobulinemia and chronic active hepatitis. [18] It is important to differentiate FPP from RTA as both the diseases may have a similar clinical picture; however, presence of tetany, cardiac arrhythmia and hypokalemia during the interictal period suggests secondary hypokalemia. It is important to differentiate RTA from FPP because during acute attack, administration of sodium bicarbonate in FPP would facilitate intracellular potassium flux and fatal hypokalemia may occur. [1] In FPP oral potassium and acetazolamide are useful in preventing the attacks but acetazolamide is contraindicated in RTA as it produces acidosis. Acknowledgment We thank Mr. Rakesh Kumar Nigam for secretarial help. References
Copyright 2010 - Neurology India The following images related to this document are available:Photo images[ni10022f1.jpg] |
| |||||||||

{kind=link}