 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 58, No. 1, January-February, 2010, pp. 112-114 Case Report Cardioembolic stroke on unaffected side during thrombolysis for acute ischemic stroke Arun Garg, Amitabh Yaduvanshi, Kapil Dev Mohindra Department of Neurology, Max Balaji Hospital, Patparganj, Delhi, India Correspondence Address: Dr. Arun Garg, Head - Stroke Neurology, Institute of Neurosciences, Medanta The Medicity, Gurgaon (Delhi NCR), Haryana - 122 001, India, gargarungarg@hotmail.com Date of Acceptance: 02-Nov-2009
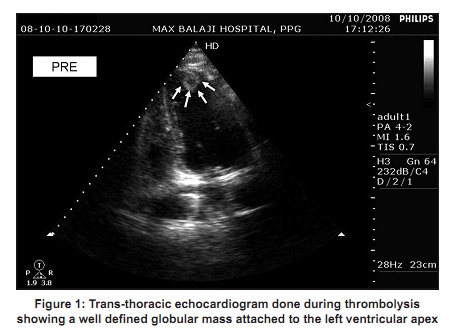
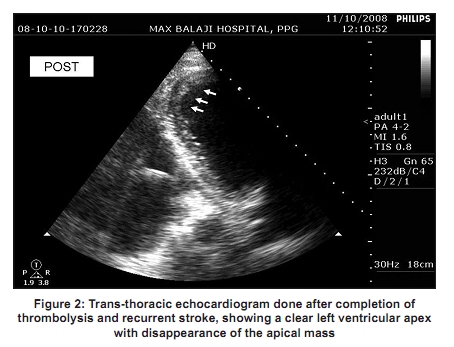
Code Number: ni10024 DOI: 10.4103/0028-3886.60419 Abstract Cardiac thrombus is not an established contraindication to thrombolysis with intravenous tissue plasminogen activator in acute ischemic stroke. Recurrent ischemic stroke involving an initially unaffected arterial territory during the course of thrombolysis in stroke has been reported, but remains exceptionally rare. We present a case that developed cardioembolic stroke on the previously unaffected side during thrombolysis for acute ischemic stroke.Keywords: Cardiac thrombus, stroke, thrombolysis Introduction Presence of cardiac thrombus is not a contraindication for intravenous thrombolytic therapy in acute ischemic stroke. However, systemic embolization shortly after thrombolytic therapy in patients with cardioembolic stroke has been reported, presumably caused by the dislodging of a preexisting cardiac thrombus. These reports, however, lacked confirmatory evidence, and the assumption was made only in retrospect. [1] We report a case of cardioembolic stroke on unaffected side during thrombolysis for acute ischemic stroke due to thrombolysis of preexisting left ventricular thrombus, confirmed by serial echocardiograms. Case Report A 72-year-old nondiabetic, normotensive male with a history of coronary artery disease, presented with right sided weakness and difficulty in speaking of 90 minutes duration. On examination he had right hemiparesis with Broca′s aphasia and his National Institute of Health Stroke Scale (NIHSS) score was 12. Computed tomography (CT) scan of head was normal. His blood pressure, sugar level, prothrombin time and platelet counts were normal. His ECG revealed bifacsicular block, but cardiac enzymes were normal. There was no history of myocardial infarction in the past. Patient was thrombolyzed with tissue plasminogen activator (tPA), 0.9 mg/kg. During the course of thrombolysis patient showed remarkable recovery and NIHSS score improved by 10 points. Two dimensional echocardiography (2D Echo) was done while infusion of tPA was still on. It revealed a thromus in the left ventricular apex [Figure - 1]. By the time thrombolytic therapy was completed, patient′s sensorium deteriorated suddenly and he developed left hemiplegia, NIHSS score of 22. Patient was intubated and put on ventilator. Repeat CT scan revealed large infarct in right middle cerebral artery (MCA) territory. A repeat 2D Echo showed disappearance of left ventricular thrombus [Figure - 2]. These observations suggest that the patient developed cardioembolic stroke on the unaffected side due to dislodgement of cardiac thrombus by thrombolytic therapy. Patient died of cardiopulmonary complications on the 10 th day of ictus. Discussion Thromboembolic complications have been observed in 1.5% of patients receiving thrombolysis for acute myocardial infarction, who were believed to have a preexisting clot. [2] Very few data are available to evaluate the risk to benefit ratio of thrombolysis in stroke patients with cardiac thrombus. One study reported five patients with cardiac thrombus who were given intravenous tPA for stroke. [3] No early systemic or cerebral embolism occurred in any of the patients. One patient had later developed recurrent cerebral embolism and died. Recurrent cerebral embolus, embolic myocardial infarction, and lower limb embolism have also been reported in cases subjected to intravenous thrombolytic therapy for ischemic stroke. [4],[5] However, diagnosis in all these patients could not be proved and was based on the temporal relation of the event following thrombolysis. Our patient developed cardioembolic stroke immediately after completion of thrombolytic therapy and we could demonstrate disappearance of pre-existing cardiac thrombus. The embolic potential of left ventricular thrombus may be directly related to duration of its formation, as recently formed, poorly adherent thrombus is more likely to dislodge. The morphology of thrombus can also help to predict subsequent embolization. Thrombus protrusion and mobility, especially those related to a recent myocardial infarction, are associated with an increased embolic risk. [6] It should, however, be emphasized that patients should not be denied the benefits of thrombolytic therapy and potential reduction in morbidity and mortality that can be achieved with this treatment, unless the associated risks are appreciable. Cases have been reported where patients with cardiac thrombus were given intravenous tPA for acute ischemic stroke without complications. [7] Even in this patient, there was a very quick and remarkable recovery; he improved 10 points on NIHSS (the "Lazarus effect") during thrombolysis before he deteriorated because of cardioembolic stroke on the unaffected side. It should also be noted that tPA induces a secondary activation of coagulation cascades which might contribute to vessel reocclusion or recurrent stroke. Cases have been reported where patients even developed intracardiac thrombus following systemic thrombolysis for stroke. [8] For selected stroke patients, for whom intravenous thrombolysis is not safe, intra-arterial thrombolysis (IAT) may be an effective treatment option. It permits a smaller dose of fibrinolytic agent to reach a higher local concentration than that reached by systemic infusion and ideally allows more complete recanalization with lower total doses of thrombolytic agent. With the smaller dose, complications from systemic fibrinolytic effects can theoretically be reduced. By eliminating the need for thrombolytics, mechanical thrombectomy has made endovascular treatment feasible in many circumstances in which IAT has been previously judged unsafe. These situations are not infrequent and include recent surgery, contralateral strokes, significant hemorrhage and abnormal hemostasis. In patients with cardiac thrombus also, mechanical thrombectomy may prove to be a safe and effective option. The major disadvantages of these endovascular recanalization techniques include relative complexity of the procedure, the level of required technical expertise, its relatively low availability, excessive trauma to the vasculature leading to vasospasm, dissection or rupture, and fragmented thrombus causing distal embolization into previously unaffected territories. [9] Nevertheless, the advantages of mechanical stroke therapy appear to significantly outweigh its disadvantages and risks, as reflected in the results of three different multicenter trials. Mechanical Embolus Removal in Cerebral Ischemia (MERCI) trial was a prospective single-arm multicenter trial designed to test the safety and efficacy of the MERCI clot retrieval device to restore the patency of intracranial arteries in the first eight hours of an acute stroke. Of the total 141 patients in whom device was deployed, recanalization was achieved in 48% (thrombolysis in myocardial infarction [TIMI] score 2-3). Clinically significant procedural complications occurred in 10 (7.1%) patients. Three cases of embolization of a previously uninvolved vascular territory occurred. Symptomatic intracerebral hemorrhage (SICH) was observed in 11 (7.8%) patients. The overall rates of good outcomes and mortality at 90 days were 27.7% and 43.5%, respectively. Good neurological outcomes at 90 days were more frequent (46% versus 10%) and mortality rate were lower (32% versus 54%) with successful compared with unsuccessful recanalization. In multi MERCI trial, the device was deployed in 164 patients. Successful recanalization (TIMI 2-3) was achieved in 55% patients with retriever alone and in 68% patients after adjunctive therapy (IA tPA). Clinically significant procedural complications occurred in 5.5% of the patients and SICH occurred in 9.8% of patients. The overall rates of good outcomes (36%) and mortality (34%) at 90 days were substantially improved in comparison with those in the MERCI trial. In Penumbra stroke trial, complete or partial revascularization occurred in 81.6% of the occluded vessels. The rate of procedural serious adverse events was 3.2%, none of which was device-related. SICH occurred in 11 out of 125 patients (11.2%), and asymptomatic ICH in 21 patients (16.8%). [10] These results were well duplicated in a post market retrospective review of 139 cases who were treated with the device at seven international centers, reflecting a favorable safety and effectiveness profile in a real-world setting. [11] Till date, limited consensus exists as to appropriate treatment of stroke in a patient with cardiac thrombus. Endovascular stroke therapy continues to evolve and improve. New recanalization strategies that may further improve what is presently available are being tested. References
Copyright 2010 - Neurology India The following images related to this document are available:Photo images[ni10024f1.jpg] [ni10024f2.jpg] |
| |||||||||

{kind=link}
{kind=link}