 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 58, No. 1, January-February, 2010, pp. 115-117 Case Report Intrathecal baclofen pump implantation in a case of stiff person syndrome Bobby Varkey Maramattom Department of Neurology, Lourdes Heart Institute and Neuro Centre, Kochi, Kerala, India Correspondence Address: Dr. Bobby Varkey Maramattom, Department of Neurology, Lourdes Heart Institute and Neuro Centre, Kochi, Kerala, India, bobvarkey@gmail.com Date of Acceptance: 02-Nov-2009
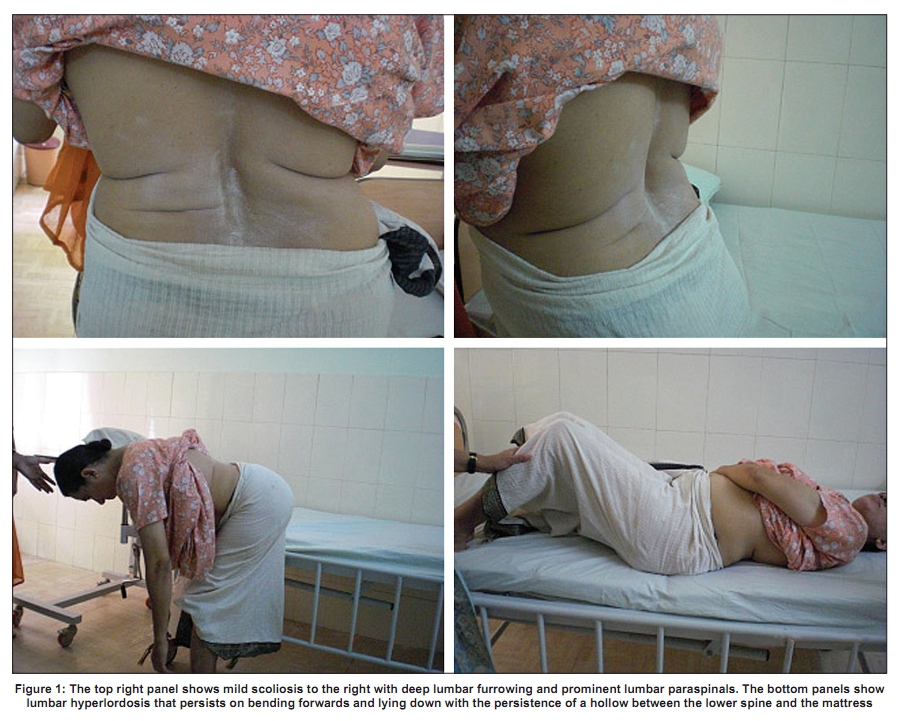
Code Number: ni10025 DOI: 10.4103/0028-3886.60420 Abstract Stiff person syndrome (SPS) is a rare disorder characterized by severe axial and/or limb rigidity, spasms and continuous motor unit activity on EMG. Symptomatically these patients are usually treated with GABAergic medications. We present a 45-year-old woman with SPS, who failed high dose of GABAergic medication. With intrathecal baclofen by intrathecal baclofen pump she had a significant improvement in her symptoms and quality of life.Keywords: Intrathecal baclofen pump, stiff man syndrome, stiff person syndrome Introduction Stiff person syndrome (SPS) is a rare progressive disorder characterized by severe axial and/or limb rigidity, spasms, and continuous motor unit activity on electromyography (EMG). [1] The estimated incidence of SPS in one in a million. Different authors have proposed different classifications for SPS based on clinical characteristics and antibody profile. Barker and colleagues [2] have classified SPS into three types: Progressive encephalomyelitis with rigidity, stiff man syndrome (SMS), and stiff limb syndrome (SLS). Progressive encephalomyelitis with rigidity is a fulminant condition characterized by widespread rigidity and death usually occurs within four months of onset. Stiff man syndrome is characterized by rigidity and painful spasms of the lumbar paraspinal, abdominal and proximal leg muscles with Lumbar hyperlordosis and often associated with anti-GAD antibodies and concurrent autoimmune disease such as insulin-dependent diabetes mellitus (IDDM) and thyroditis. Stiff limb syndrome is characterized by rigidity, spasm and abnormal posturing of a distal limb, usually the leg, simulating dystonia. The other classification proposed by Grimaldi and colleagues divides SPS into three types: Type I, associated with other autoimmune diseases and often anti GAD +ve (55-60% of patients); Type II: Paraneoplastic, anti amphiphysin positive (5% of patients); and Type III: Idiopathic, antibody negative (35-40% of patients). [3] Only a few cases of SPS have been reported from India. [4],[5],[6],[7] Though most patients are treated with GABAergic medications, only few achieve a satisfactory quality of life (QoL). Intrathecal baclofen (ITB) pump therapy has been tried in a few patients with benefit. However, its use remains sporadic. We report ITB use in an Indian patient with SPS and discuss issues pertinent to our country. Case Report A 45-year-old woman presented with pains in both legs and difficulty in walking of four years duration. Her dominant symptoms were stiffness and pain in both legs and lower back. She had a history of occasional falls related to sudden spasms in the legs precipitated by loud sound. She sustained a recent left patellar fracture after a fall. She was admitted with an acute exacerbation of stiffness and pain. For the past three years she had required assistance for all activities of daily living. She had diabetes for which she was on insulin. On examination, she had hyper lumbar lordosis with rock hard lumbar paraspinal muscles and deep lumbar furrowing [Figure - 1]. Both legs were stiff (left more than right) and there was clawing of the left toes [Ashworth scale 5]. Motor and sensory examination was normal. Her gait was slow, cautious and ′tin soldier′ like. Anti GAD antibodies were negative and MRI of the spine was normal. Nerve conduction studies were normal. EMG studies showed continuous motor unit activity from the lumbar paraspinal muscles. A paraneoplastic work up was negative. She was diagnosed as SMS variant of SPS. She was treated for two weeks with high dose of oral diazepam (90 mg/day), oral baclofen (90 mg/day) and continuous IV infusion of diazepam (50 mg/ day). Methylprednisolone was deferred because of brittle diabetic state and the patient was unwilling for plasma exchange. She had little improvement in stiffness but was extremely sedated. After two weeks, the option of ITB pump was offered for which she agreed. A test dose of ITB (50 mcg) dramatically reduced her stiffness, following which she opted for ITB pump implantation. Accordingly a Medtronic Synchromed II ITB pump was implanted with the intrathecal catheter tip placement at T8 level with an initial ITB dose of 50 mcg/day. Postoperatively, she showed good improvement in stiffness and pain. After 10 days, her doses of oral medications could be reduced to 10 mg of diazepam bedtime. At the last follow-up, two months, her ITB dose was readjusted to 200 mcg/day and a diazepam dose of 10 mg/day. Her gait and stiffness improved subjectively by 70-80% [Ashworth scale 2] and spasms disappeared. She became independent for all activities of daily living. Discussion The SMS variant of SPS is the most amenable to benzodiazepines and other GABA enhancing drugs such as vigabatrin, valproate, tiagabine, gabapentin or baclofen, but the doses required often cause unacceptable side effects. Antibodies against glutamic acid decarboxylase can be detected in some patients. GABA (A)-receptor-associated protein (GABARAP) is a novel protein that is responsible for the stability and surface expression of the GABA (A)-receptor. Up to 65- 70% of SPS patients demonstrate GABA (A)-receptor associated protein antibodies. [8] These GABARAP antibodies significantly inhibit the surface expression of GABA(A)-receptor and thus impair GABAergic pathways. Some patients require periodic plasma exchange, intravenous immunoglobulin or high dose steroids for symptom relief. [9] However, there are some inherent problems with these treatment modalities. Plasma exchanges require periodic visits and hospitalization for 5-10 days and IVIG is extremely expensive. The cumulative cost of PE and IVIG over time can outstrip that of ITB pump implantation and refill. ITB pump implantation has been shown to improve symptoms in some patients with SPS. [10] The advantages of ITB pump include a targeted baclofen delivery into the intrathecal space which delivers a continuous 24/7 GABAergic therapy and reduces spasms and stiffness at approximately 1/500 th the oral dose of baclofen thus minimizing sedation and systemic side effects. The disadvantages include rare instances of catheter infection, catheter leakage or pump failure with catastrophic muscle spasms and rhabdomyolysis and multiorgan failure. [11] The cost of a Medtronic synchromed II pump is approximately Rs 3 lakh and the cost of implantation is roughly Rs 25,000. The ITB pump holds 40 ml of baclofen. Depending upon the patient′s requirement for baclofen the refill interval can vary from 30-90 days. Each refill costs the patient approximately Rs 24-36,000 per year. The pump lasts for an average of seven years after which it has to be replaced. Thus economically ITB pumps may be beyond the reach of many Indian patients. Although ITB pump implantation is an expensive option, our case report highlights the option of considering it in selected cases of SPS to improve the quality of life. References
Copyright 2010 - Neurology India The following images related to this document are available:Photo images[ni10025f1.jpg] |
| |||||||||

{kind=link}