 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 58, No. 1, January-February, 2010, pp. 118-121 Case Report Progressive multifocal leukoencephalopathy in a patient with idiopathic CD4+T lymphocytopenia Vinod Puri, Neera Chaudhry, Parveen Gulati 1 , Nisheeth Patel, Medha Tatke2 , Sanjiv Sinha3 Departments of Neurology, 2 Pathology and 3 Neurosurgery, G. B. Pant Hospital, New Delhi - 110 002, Correspondence Address: Dr. Vinod Puri, 15, Type VI, MAMC Campus, Kotla Road, New Delhi - 110 002, India, vpuri01@gmail.com Date of Acceptance: 29-Oct-2009
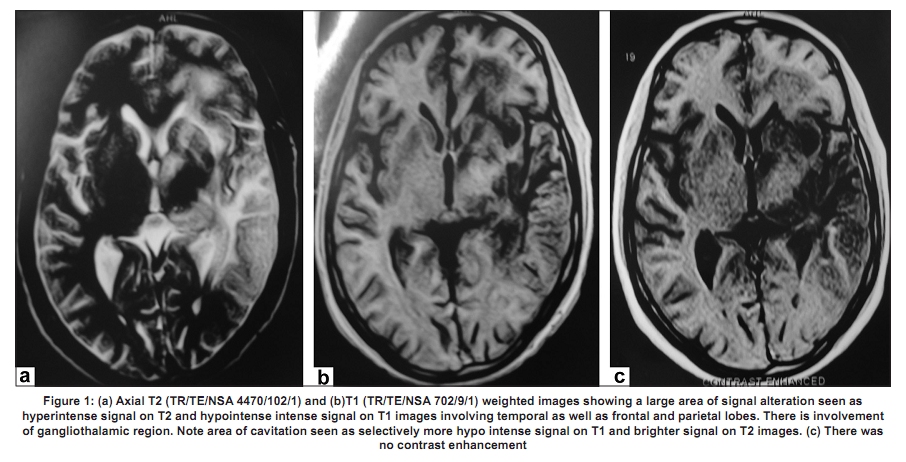
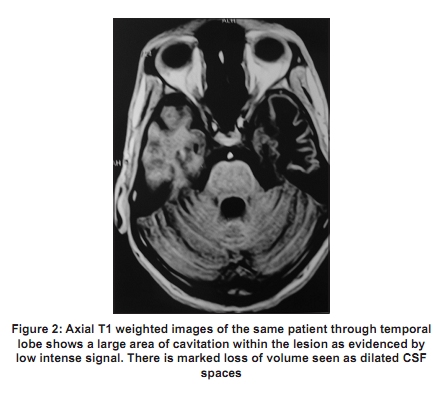
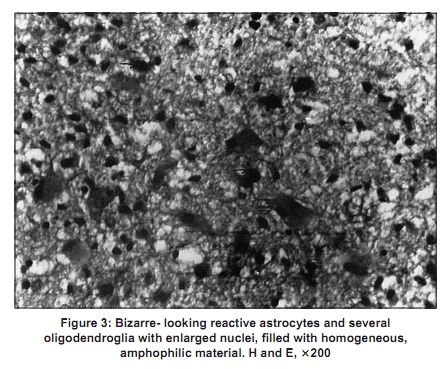
Code Number: ni10026 DOI: 10.4103/0028-3886.60423 Abstract Progressive multifocal leukoencephalopathy (PML) is demyelinating of central nervous system caused by JC virus infection and often occurs in immunodeficient individuals. We report progressive PML in a 30-year-old male with idiopathic severely depressed CD4+T lymphocyte count. He was sero-negative for human immunodeficiency virus (HIV) infection.Keywords: Progressive multifocal leukoencephalopathy, idiopathic CD4+T lymphocytopenia, HIV infection Introduction Progressive multifocal leukoencephalopathy (PML) is a demyelinating disease of the central nervous system caused by JC virus infection. The clinical characteristics include dementia, dysphasia, focal neurological deficits and the course is inexorably progressive course. Histopathological characteristics include demyelination, bizarre astrocytes with lobulated hyperchromatic nuclei and enlarged oligodendroglial nuclei containing viral inclusions. PML mostly occurs in immunodeficient individuals in particular in patients with acquired immunodeficiency syndrome (AIDS) [1] and rarely in patients with idiopathic CD4+ lymphocytopenia (ICL). [2],[3] We present histologically proven PM in a patient with ICL. Case Report A 30-year-old male presented with progressive cognitive decline characterized by an impairment of recent memory, naming difficulty, errors in financial transactions and a change in personality of three months duration. Two months after the onset of initial symptoms, he developed sudden onset right sided weakness and subsequent disturbances in language functions, over the next ten days. Neurological examination revealed a conscious person with posterior aphasia. Detailed cognitive function evaluation was not possible. He had right upper motor neuron facial palsy and right hemiplegia with motor power of grade 3-4/5. Deep tendon jerks were brisk on the right side, with extensor plantar. Examination of other systems was essentially normal. Laboratory investigations: Erythrocyte sedimentation rate (ESR) was 66 mm in the first hour, ELISA for human immunodeficiency virus (HIV) was non-reactive on three occasions and on Western blot analysis no viral specific bands for HIV-1 or HIV-2. White blood cell (WBC) count was 7400/µl (normal, 3900-1140/µl) with absolute lymphocyte count of 1406 µl (normal, 1000-3500/µl);. % of lymphocytes 19% (normal, 26-48%); absolute CD3+ cells: 982/µl (normal, 740- 2400/ µl), % of CD3+ cells-69.84% (normal, 57- 85%); absolute CD4+ cells-81/µl (normal, 440-1600µl), % of CD4+ cells-8.30% (normal, 29-61%); absolute CD8+ cells- 769/µl (normal, 170-940 µl), % CD8+ cells-78.25% (normal, 11-39%); CD4+/CD8+ ratio 0.11 (normal, 0.9-5). Serum immunoglobulin profile was IgG 597 mg/dl (normal, 800-1800 mg/dl), IgA 106 mg/dl (normal, 100-490 mg/dl), and IgM 28 mg/dl (normal, 60-280 mg/dl). Hepatitis B surface antigen was non reactive. Serology for cytomegalovirus, Ebstein-Barr virus, herpes virus and toxoplasma were negative. EEG showed diffuse slowing of the back ground activity and focal polymorphic delta activity over the left temporal region and no periodic discharges. Magnetic resonance imaging (MRI) of brain [Figure - 1] and [Figure - 2] showed a large area of signal alteration in left temporal lobe extending to parietal as well as frontal lobe, hyper intense on T2 and heterogeneously hypointense intense on T1 weighted images. An area of cavitation within the lesion in the temporal lobe, as well as a marked loss of volume of the temporal lobe was also seen. No contrast enhancement on gadolinium was observed, nor was there any mass effect. An open brain biopsy [Figure - 3] revealed foci of demyelination infiltrated with numerous fat laden macrophages, reactive bizarre hypertrophic astrocytes, and oligodendrocytes with large amphophilic nuclei. The patient was managed conservatively by supportive care, but he had a rapid downhill course and died within three months of onset of illness. Discussion In PML the target of the polyoma virus JC (JCV) is oligodendrocyte of the central nervous system, the cell that forms and maintains the myelin sheath, is its target. [4] Prior to HIV epidemic, PML most commonly was described in patients with lympho-proliferative disorders, myelo-proliferative diseases, and chronic infectious or granulomatous diseases. In the recent years PML is mostly described in patients with AIDS, 55 to 85%. The incidence of PML in patients with HIV infection is about 4%. [5] However, the clinical characteristics of PML are identical in both HIV and non-HIV patients. [6] There are anecdotal case reports of PML in patients with hyper immunoglobulin E recurrent infection syndrome (HIES) [7] and ICL. [2],[3] ICL is an extremely rare syndrome and characteristics include a CD4+ count that is less than 300 cells/cumm, or a CD4+ count that is < 20% of total T cell count on two occasions, with no evidence of HIV infection on testing, and absence of any defined immunodeficiency or therapy that depresses the levels of CD4+ T cells. [8] There are certain differences in immunologic profile in patients with ICL and HIV infection. In ICL there is lymphocytopenia, occasional decrease in CD8+ counts and low or normal level of immunoglobulins, whereas in HIV infection patients there is hypergammaglobulinemia. In the present case, the CD4+ cells were consistently low (on three occasions) with low serum immunoglobulin levels. Other CNS complications reported in patients with ICL include: Undefined dementia, encephalopathy, [9] epilepsy, [8] intracranial hemorrhage, [10] paraparesis, [11] and opportunistic infections like disseminated tuberculosis, [12] cryptococcosis, toxoplasmosis and histoplasmosis. [8],[13],[9] There are anecdotal reports of its association with lymphoproliferative disorders like leptomeningeal non- Hodgkin lymphoma. [14] The etiology of ICL remains unclear. It is believed that this condition may occur as a result of the inherent variability of T lymphocyte subsets [15] and that it represents the tail end of natural statistical variation in CD4+ cell counts. [16] Two familial cases have also been reported. [13],[17] In the present case, the CD4+ cells were consistently low (on three occasions) with low serum immunoglobulin levels. The common clinical features of PML include visual field deficit (45%) and altered mental functions [dementia, confusion, and personality change] (38%). Motor weakness may not be present early but eventually occurs in 75% of the cases. [15] Less frequent features include vertigo, seizures, headache, and aphasia. [1] Spinal cord involvement is rare. It has a relentlessly progressive course, with death often occurring within nine months of the onset of symptoms. However, some HIV associated patients have shown dramatic clinical improvement with up gradation of their immune status after institution of highly active antiretroviral therapy. [5] Critical analysis of the course of PML in patients with ICL does not suggest that the course of the PML is not influenced by the underlying immunodeficiency state. [2] Only one patients with PML and ICL with a survival of three years has been reported. [3] MRI is the imaging modality of choice, with greater sensitivity than CT [4],[18] and shows multifocal asymmetric, white matter lesions, hyper-intense on T2 weighted images and hypo-intense on T1 weighted images. These lesions mostly do not enhance on contrast however, enhancement can be seen in 5-10% of the cases. Contrast enhancement of the lesions has a prognostic significance. It suggest a more robust immune response to the viral antigens and suggests likely long term survival. [19] The lesions are often bilateral, rarely can be unilateral. [4],[18] The lesion location is periventricular and at the gray white interface, involving the U fibers thus giving a scalloped appearance. The parieto-occipital and frontal locations are most common and approximately one third of cases have some involvement of the posterior fossa, though other lobes may also be involved. Isolated infratentorial involvement is found in about 10% of cases. [19] Involvement of small myelinated fibers that course through the basal ganglia and adjacent structures results in the involvement of these structures. [18] On autopsy, the demyelinating lesions are mostly multifocal and range from 1 mm to several centimeters, larger lesions being the result of coalescence of smaller lesions. [20] The confluent lesions may cavitate. [21] The extensive lesion in the present case could be due to coleasence of smaller lesions with an eventual cavitation. The clinical as well as the histopathological profile of our patient was that of PML. Our patients had many unusual MRI features: Unilateral extensive lesion, temporal location, and early cavitation. These unusual features on MRI may have to do something with the underlying immunodeficiency state. ICL. However, the clinical course was similar to PML in other immunodeficiency states. We emphasize that in patients with clinical and imaging features suggestive of PML and with no obvious immunodeficiency state should be investigated for ICL. References
Copyright 2010 - Neurology India The following images related to this document are available:Photo images[ni10026f3.jpg] [ni10026f2.jpg] [ni10026f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}