 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 58, No. 1, January-February, 2010, pp. 122-124 Case Report Non-traumatic intraosseous cerebrospinal fluid cyst with associated craniovertebral anomalies: A case report and suggested mechanism of formation Tony Abraham Thomas, Damodar Rout Department of Neurosurgery, Sri Ramachandra University, Chennai, India Correspondence Address: Dr. Tony Abraham Thomas, Department of Neurosurgery, Sri Ramachandra University, No. 1 Ramachandra Nagar, Porur, Chennai - 600 116, India, tonyabthomas@gmail.com Date of Acceptance: 29-Oct-2009
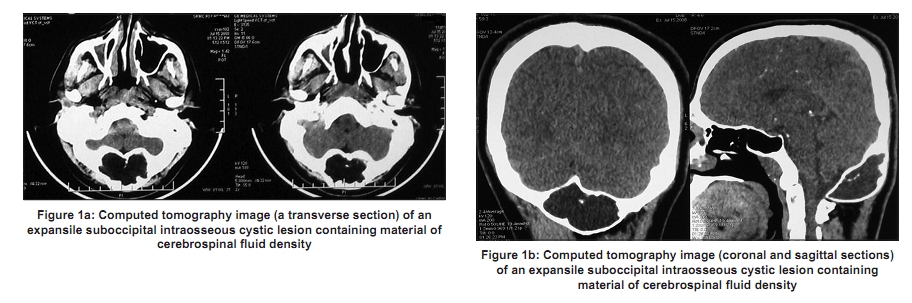
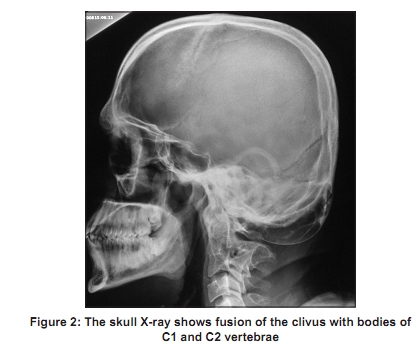
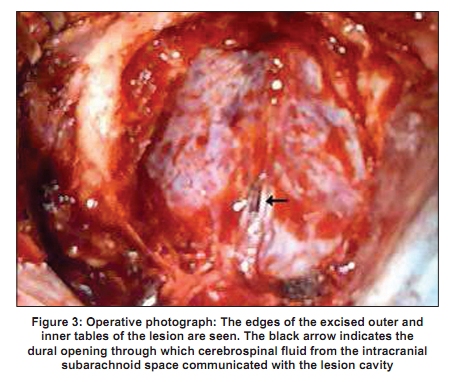
Code Number: ni10027 DOI: 10.4103/0028-3886.60424 Abstract Intraosseous cerebrospinal fluid (CSF) cysts, also known as intra-diploic arachnoid cysts, are usually of post-traumatic origin. Lesions presenting without a history of trauma are rare and are presumed to be of congenital origin. We report a young man with an intraosseous cystic lesion containing CSF and communicating with the intracranial subarachnoid space through a dural opening. The presence of other congenital defects of the skull and spine could be a pointer in this direction. Surgical management involves craniectomy and repair of the dural defect followed by cranioplasty for the bony defect.Keywords: Arachnoid cyst, intraosseous cerebrospinal fluid-cyst, intradiploic, intraosseous Introduction Intraosseous cranial lesions can result from a wide range of pathological conditions. An intraosseous cerebrospinal fluid (CSF) cyst is an uncommon differential diagnosis for such lesions. Intraosseous CSF-cysts are usually associated with post traumatic growing skull fractures. Cystic lesions of the bone containing CSF of a non-traumatic origin are rare and are presumed to be of congenital origin. Literature search revealed report of five such cases and on small series of five cases. [1],[2],[3],[4],[5],[6] To our best of knowledge, there have been no cases associated with congenital craniovertebral bony anomalies. We report a young adult with a slowly growing intra-osseous cystic lesion containing CSF and concomitant bony craniovertebral anomalies. Case Report A 25-year-old man presented with a history of a progressively enlarging swelling in the occipital region since childhood and occipital headache of seven years duration. There was no history of trauma and significant family history. On examination, there were no neurological deficits. There was a suboccipital, midline bony swelling measuring 8 x 5 cm. He had restricted jaw opening and a mild torticollis. Computed tomography (CT) of brain showed an intraosseous irregular expansile lesion in the occipital bone in the midline, with scalloping and thinning of both outer and inner tables. The lesion extended up to the foramen magnum and laterally up to the condylar region [Figure - 1]. Plain skiagram of the skull and cervical spine showed occipitalization of the atlas and Klippel-Feil anomaly with anterior fusion of the clivus, anterior arch of atlas and C2 vertebrae [Figure - 2]. During surgery, the posterior arch of atlas was found to be hypoplastic on right side and occipitalized on the left. The outer table was found to be papery thin, bluish in appearance at places and bulging outwards. On opening the outer table, it was found to contain CSF. The inner table had also been thinned out by the lesion. There was a small elliptical dural opening measuring about 4 mm long, in the midline, through which CSF was found gushing out with each pulsation [Figure - 3]. The dural opening was closed primarily after excision of the thinned-out bone. A cranioplasty was done using acrylic bone cement to cover the defect. At six months follow-up, he was free of headache. Discussion The differential diagnosis for a bony cystic lesion of the cranium includes intraosseous epidermoid/dermoid cyst, aneurysmal bone cyst, fibrous dysplasia, eosinophilic granuloma, hydatid cyst and malignant conditions like plasmacytoma, myeloma, osteogenic sarcoma and intraosseous meningioma. Eosinophilic granuloma and neoplasms are osteolytic rather than expansile lesions and their contents are not of CSF density. Fibrous dysplasia cystic lesions are usually very small and multiple with attendant sclerosis of bone. Magnetic resonance imaging (MRI), especially with fat suppression sequences can help to eliminate epidermoid and dermoid from the list and further elucidate the nature of the contents. The possible differentials for an intraosseous expansile cystic bony lesion with contents of CSF density similar to the case described can be narrowed down to aneurysmal bone cyst and hydatid cyst. Intraosseous CSF cyst is an uncommon diagnosis that needs to be considered. The terms arachnoid cyst, leptomeningeal cyst and CSF-fluid fistula have been used synonymously in previous reports to describe these cysts. They have been often referred to as being intradiploic in position. These cysts are not entirely between the two tables of the skull as they almost always have a communication with the intracranial subarachnoid space. Moreover, the surrounding bone is so thinned out that it is not clear if they are strictly intra diploic in position based on radiological and per-operative findings. Since the cyst is intraosseous in location, contains CSF and is in communication with the intracranial subarachnoid space, the term ′intraosseous CSF cyst′ would be, in our opinion be more appropriate. Intraosseous cyst containing CSF in association with post-traumatic growing fracture [7,8] of the skull is a well documented condition. Occurring almost exclusively in children, these cysts result from continuous wedge pressure through a fracture line driving arachnoid membrane and CSF into the diploic space of the skull. CSF cysts of non-traumatic origin are comparatively much rarer. The commonest location for a non traumatic intraosseous CSF cyst is the midline suboccipital region. All five cases reported by Hasegawa et al. [3] were in this region. CSF cysts have also been documented in the fronto- temporal region and anterior cranial fossa. They may be asymptomatic and discovered incidentally or may present clinically as a progressively enlarging swelling with or without headache. These lesions are characteristically thin-walled due to the progressive expansion of the enclosing bone. Further expansion with erosion of the outer table of the bone has also been reported. [6] During surgery, they have been found to almost invariably communicate with the intracranial subarachnoid space through a dural opening. The opening may be single or multiple and is usually small and round or elliptical. Egress of CSF out of this opening in a pulsatile manner is seen with each pulsation of the brain. The dural opening in a CSF cyst associated with a growing fracture, on the other hand, is usually linear and its size is determined by the dimensions of the fracture. Although these lesions usually only contain CSF, small amounts of dysplastic brain tissue that has prolapsed through the opening has been reported. [3] A distinct arachnoid membrane may rarely be seen lining the lesion. The origin and pathogenesis of intraosseous CSF cysts is not clear. They are assumed to be congenital in origin. They enlarge gradually, rendering the bony wall papery thin, the pulsatile flow of CSF providing the necessary pressure head for expansion. This process, we presume, must have been initiated before the ossification of the cranium since it appears unlikely that normal CSF pressure would be enough to produce an expansile lesion in intact bone. The basiocciput ossifies in cartilage and in this case, there could have been a defect in the chondrocranium. A congenital opening in the dura may have provided a narrow vent for intracranial pulse waves to create a space in the underlying defect, which continued to expand after ossification, by a ball-valve mechanism. The patient′s history and per operative evidence are in favor of a congenital origin of the cyst. The association with craniovertebral segmentation anomalies in this case, is another pointer towards a congenital origin, though this could be coincidental. References
Copyright 2010 - Neurology India The following images related to this document are available:Photo images[ni10027f1.jpg] [ni10027f2.jpg] [ni10027f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}