 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 58, No. 1, January-February, 2010, pp. 125-127 Case Report Vertebral body hyperostosis as a presentation of Pott's disease: A report of two cases and literature review Alok Umredkar, Sandeep Mohindra, Rajesh Chhabra, Rahul Gupta Department of Neurosurgery, Postgraduate Institute of Medical Education and Research, Chandigarh, India Correspondence Address: Dr. Alok Umredkar, Department of Neurosurgery, Postgraduate Institute of Medical Education and Research, Chandigarh, India, alokumr@yahoo.co.in Date of Acceptance: 23-Oct-2009
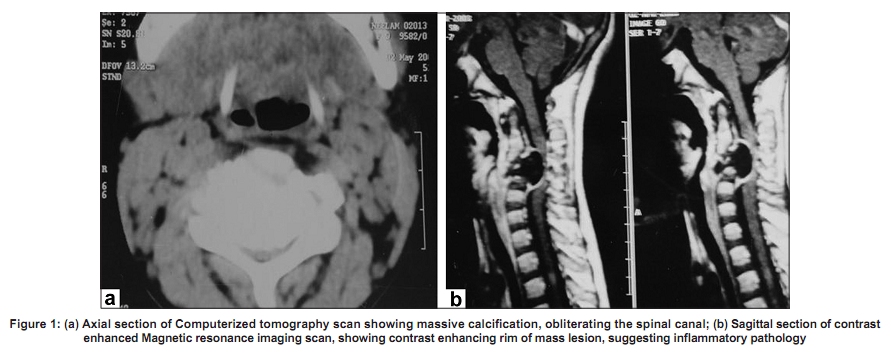
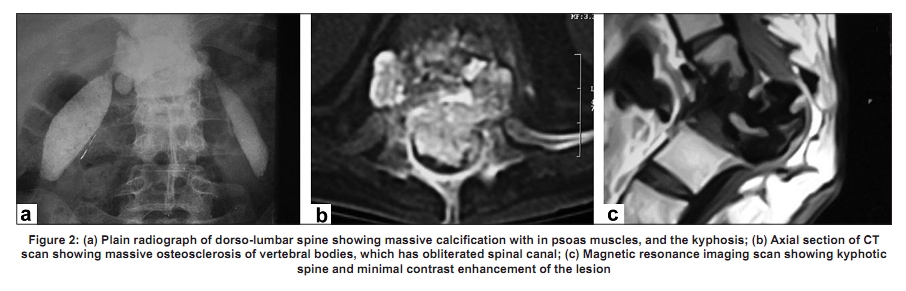
Code Number: ni10028 DOI: 10.4103/0028-3886.60426 Abstract Vertebral body tuberculosis has numerous forms of presentations. We present two patients of Pott's disease, in whom vertebral body hyperostosis was the radiological presentation. Both the patients had massive hyperostosis of vertebral bodies leading to the obliteration of the spinal canal and neurological deficits. The first case had associated lupus vulgaris, while the second patient had milliary mottling of lungs and calcified bilateral psoas muscles. Surgical decompression, followed by full-dose chemotherapy, remains the hallmark of management of this disease.Keywords: Pott′s disease, hyperos tosis, lupus vulgaris, tuberculosis Introduction Tuberculosis of spine has shown resurgence in the recent past in parallel with organ transplantation, cancer chemotherapy and immunodeficiency diseases. [1],[2] Spinal tuberculosis may produce serious neurological deficits; [3],[4] cervical involvement is rare, about 0.03%. [5] Numerous patterns of vertebral body tuberculosis include fragmentary, osteolytic, subperiosteal and localized/sclerotic. [3],[6],[7] Radiological presentation like that of malignancy has also been reported. [1],[8] Magnetic resonance imaging (MRI) and single photon emission computed tomography (SPECT) studies are helpful in detecting the disease early and in accurate anatomic localization. [9],[10] Case Reports Case 1 A nine-year-old female child, from a poor economic background, presented with gradually progressive spastic quadriparesis of three years duration. Power in upper limbs was grade 2/5, while in the lower limbs with severe spasticity. There were multiple eruptions on nose and hands, the biopsy of which revealed lupus vulgaris. Plain skiagram of cervical spine suggested a bony mass lesion involving third vertebral body. Computerized tomography (CT) scan showed a dense bony hyperostosis of vertebral body, grossly chinking the spinal canal [Figure - 1]a. Gadolinium-enhanced MRI showed rim-enhancing mass, compressing the cord [Figure - 1]b. There was no extraspinal collection. Fine needle aspiration cytology of the spinal lesion was unsuccessful due to its bony hard texture. With the provisional diagnosis of chordoma, the patient underwent decompression of cervical spine from anterior cervical approach and placement of an iliac bone graft. Plating was not done. Post-operatively, the spine was immobilized for three months with HALO. Histopathology revealed areas of destruction, with necrosis and calcification, consistent with tuberculosis. Culture was not done. Four-drug chemotherapy (isoniazid 5 mg/kg; rifampicine 10 mg/ kg; ethambutol 15 mg/kg and pyrizinamide 25 mg/kg ) was administered for 18 months. At the two-year follow-up, the patient was asymptomatic with no residual neurological deficit. Case 2 A 32-year-old female presented with a history of gibbus formation at mid back for 19 years. The patient never asked for medical help, as there was no neurological deficit. Before this admissin the patient developed paraparesis and bladder hesitancy. On examination, both limbs had power grade 4/5, with a normal tone. Plain radiograph of dorso-lumbar spine showed kyphotic thoracic spine and massive calcification, spilling all around in paraspinal region [Figure - 2]a, while chest radiograph revealed calcified hilar nodes. CT scan revealed hyperostosis of vertebral body [Figure - 2]b. MRI showed spinal deformity and hypodense lesion, with minimal contrast enhancement occupying the entire vertebral body [Figure - 2]c. After four weeks of four-drug chemotherapy administration, the bladder symptoms improved and patient could walk normally . Four-drug chemotherapy (isoniazid 5 mg/kg; rifampicine 10 mg/ kg; ethambutol 15 mg/kg and pyrizinamide 25 mg/kg) was administered for 18 months. At the two-year follow-up, the patient remained asymptomatic. Discussion Classical presentation of spinal tuberculosis is of four types; fragmentary, osteolytic, subperiosteal and localized/sclerotic. [1],[3] Unusual forms occur in 30% of cases, which include destruction of posterior arch, [11] isolated neural arch, [12] single vertebral body, or Pott′s disease without bony involvement. [4] Other uncommon variants are centrosomatic, suboccipital, subligamentar. [13] "Sclerosis" as a presentation of Pott′s spine is noted in more than half the patients, which progresses for over a year and returns to normal after two-and-a-half years of treatment. [14] Calcification within the paraspinal soft-tissue has also been reported. [15] The radiological diagnosis is important as radiographic changes are significant when final diagnosis is reached. [2] Associated extraspinal collections, identifiable on contrast MRI, are the hallmark of spinal tuberculosis, [7],[11],[13] providing a site for establishing the diagnosis. [5] British Infection Society has given specific guidelines for the diagnosis and treatment of CNS tuberculosis. [16] Pott′s disease, associated with lupus vulgaris, has been reported earlier. [17] Vertebral body hyperostosis as a presentation of Pott′s disease has not been reported earlier. Differential diagnosis of such a lesion includes osteochondroma, chondromyxoid fibroma, [18] giant cell tumor, metastases especially from prostate, locally malignant osteoblastoma, [19] chordoma, chondrosarcoma and chondroblastoma. Plain X-rays and CT scan may not differentiate between inflammatory and neoplastic pathologies, but MRI may highlight contrast-enhancing rim, suggestive of tuberculosis (as in our case), while uniformly enhancing lesion is well-demonstrated in osteochondroma. Absence of paraspinal fluid collections may further make such a differentiation difficult as in both of our cases. Non-neoplastic pathologies, which need to be differentiated, are multiple hereditary exostoses, [20] Paget′s disease and fibrous dysplasia. Pathophysiology causing vertebral hyperostosis in tuberculosis in not known. It may be a form of metastatic calcification. Such a widespread calcification may be an example of metastatic calcification, but kyphosis is rarely associated. Moreover, blood vessels, kidneys, lungs and gastric mucosa are likely involved, instead of muscles and vertebral body, with deranged calcium metabolism. In the first case, cervical vertebra and in the second case, dorsal vertebra may be examples of dystrophic calcification, where the calcium salts have deposited in non-viable bony matrix of vertebral bodies which were presented as vertebral hyperostosis. The psoas muscles were like that of ′heterotopic bone,′ where calcification had occurred in viable tissues. Conclusion Bony hyperostosis of vertebral body may be a rare presentation of Pott′s disease. Tuberculosis, being a systemic disease, should always be kept among the differential diagnoses of any unusual radiographic spinal abnormality, especially when some other organ is involved. Fine needle aspiration cytology may provide the correct diagnosis. Surgical decompression, followed by full-dose chemotherapy remains the management of choice, even today. References
Copyright 2010 - Neurology India The following images related to this document are available:Photo images[ni10028f1.jpg] [ni10028f2.jpg] |
| |||||||||

{kind=link}
{kind=link}