 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 58, No. 1, January-February, 2010, pp. 128-130 Case Report Dural based primary osteosarcoma in right fronto-temporal region with review of literature Nandita Ghosal, Ravi Dadlani 1 , Sunil V. Furtado1 , Naman Bagdi 2 , A. S. Hegde3 Departments of Pathology and Transfusion Medicine, 1 Neurosurgery, 2 Radiology, 3 Neurosciences, Sri Sathya Sai Institute of Higher Medical Sciences, Bangalore, India Correspondence Address: Dr. Nandita Ghosal, Department of Pathology, Sri Sathya Sai Institute of Higher Medical Sciences, EPIP Area, Whitefield, Bangalore - 560 066, India, nandita.g@rediffmail.com Date of Acceptance: 23-Oct-2009
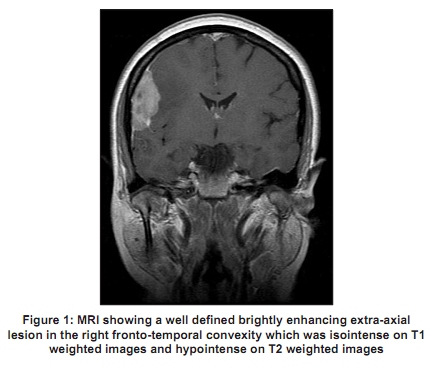
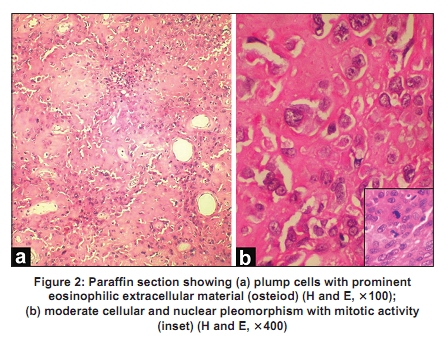
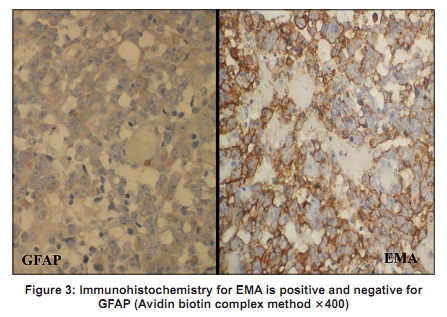
Code Number: ni10029 DOI: 10.4103/0028-3886.60428 Abstract We report a case of primary dural based osteosarcoma in the right fronto-temporal convexity in a 43-year-old female who presented with a short history of seizure and headache. Radiologic evaluation revealed a well defined brightly enhancing extra-axial lesion in the right fronto-temporal region with a dural tail around the sylvian fissure. The overlying bone was uninvolved. Paraffin section of the tumor showed plump cells with moderate nuclear and cellular pleomorphism with eosinophilic extracellular material (osteiod) between the cells. At a few places, lace like osteiod was seen encasing individual cells signifying osteiod being formed by tumor cells. Immunohistochemistry for EMA was focally positive and negative for S-100 protein and GFAP. A final histopathological diagnosis of dural based primary osteosarcoma of the right fronto-temporal region was rendered. To the best of our knowledge this will be the eighth such case in literature.Keywords: Central nervous system, dura, extraskeletal osteosarcoma, fronto-temporal Introduction Osteosarcoma rarely affects the skull; such cases constitute fewer than two per cent of all osteosarcomas. [1] Osteosarcomas that originate from the meninges are exceedingly rare. [2] We present one such rare case of primary dural based osteosarcoma in the right fronto-temporal region in a 43-year-old female. Case Report A 43-year-old female was admitted to our hospital with history of generalized tonic clonic seizures of six months and generalized headache of three months duration. Patient had no neurological deficits on examination. Magnetic resonance imaging (MRI) with contrast revealed a well defined uniformly enhancing extra-axial right fronto-temporal lesion measuring 3.9 x 3.6 x 2 cms overlying the sylvian fissure. The lesion was isointense on T1 weighted images and hypointense on T2 weighted images with a dural tail. Central nonenhancing areas of calcification were present [Figure - 1]. There was mass effect and perilesional edema. There was no evidence of infiltration of the overlying bone. A radiological diagnosis of a meningioma was given. The patient underwent a right frontotemperoparietal craniotomy with near total excision of the tumor. Per-operatively the tumor was firm and fleshy in consistency. Overlying bone was not involved. There was focal infiltration of the underlying cortex. A peroperative diagnosis of enplaque meningioma was made. Tissue was sent for histopathological evaluation. Five micron thick sections were cut and stained with hematoxylin and eosin. Microscopic examination revealed a tumor composed of plump oval cells with a nucleus showing prominent chromocentres [Figure - 2]a. The cells showed moderate amount of nuclear and cellular pleomorphism with a few tumor giant cells. A prominent eosinophilic lace like extracellular material (osteiod) was seen laid in between the cells as well as surrounding individual cells [Figure - 2]b. Mitotic figures were identified [[Figure - 2]b (inset)] along with hypercellular areas. A single focus showed a small bit of brain parenchyma with focal infiltration of tumor into it. No meningothelial whorls or psamomma bodies were identified. Immunohistochemistry (Avidin Biotin Complex method) for glial fibrillary acidic protein (GFAP) and S-100 protein were negative. A focal positivity for epithelial membrane antigen (EMA) was noted [Figure - 3]. On the basis of the histomorphological features a diagnosis of primary dural based osteosarcoma of the right fronto-temporal region was rendered. A thorough metastatic workup and the subsequent follow-up yielded no additional evidence of osteosarcoma in any other site. Discussion Primary sarcomas of the brain constitute < 0.1% of primary intracranial neoplasms. [3] Intradural POS is exceedingly rare, and to our knowledge, only five cases [4] have been cited in the modern literature. POS arising from the meninges are very uncommon tumors. [5] A review of the literature yielded only 17 additional cases of primary osteosarcomas of the brain in humans and were reported between 1941 and 2008. [6],[7],[8],[9],[10],[11],[12] Of these, seven were dural based [Table - 1] and nine were totally intra-axial. The different sites were one in frontal location, one bifrontal, four frontoparietal, one in temporal convexity and one in frontodorsal. Although radiotherapy is known to be a causative factor for the development of osteosarcomas, only two cases of meningeal osteosarcomas after radiotherapy have been reported. [6],[13] To the best of our knowledge, meningeal osteosarcoma has not been described in the context of metastasis from remote bone tumors. However, Ashkan et al. [14] described a case of metastatic osteosarcoma to the cerebellum from a primary in the femur. It is thought that the meninges contain multipotential mesenchymal cells that may be the origin of sarcomas of various differentiations. [15] This fact may also explain the observation of mixed mesenchymal differentiation, such as osteoid, cartilaginous, and osseous tissue in meningeal tumors. Given the presumed origin of the sarcomatous elements of a gliosarcoma, we postulate that the current tumor arose from mesenchymal components such as perivascular sheath of blood vessels in the sylvian fissure or overlying dura. [16] The exact cause of these rare lesions remains uncertain. The main differential diagnosis of meningeal osteosarcoma comprises anaplastic meningioma, sarcomatous tumors of the meninges and a gliosarcoma. Use of the term meningeal sarcoma in reference to meningeal based sarcomas should be abandoned in favor of specific sarcoma classification. In the present case there were no meningothelial whorls or psammoma bodies. In addition the whole tumor was showing presence of osteiod along with foci where individual cells were surrounded by thin lace like osteiod suggesting the tumor cells forming the osteiod. Although there was focal positivity for EMA, we rendered diagnosis of primary osteosarcoma as there was not a single area which resembled meningioma and the whole tumor showed histomorphology of osteosarcoma. Review of literature showed that some of the osteosarcoma can show cytokeratin as well as EMA positivity. [17],[18] Lindang et al. [17] found EMA positivity in 13 of the 25 cases of cases extraskeletal osteosarcoma. A negative immunohistochemistry with GFAP ruled out gliosarcoma. Recent studies have shown that a combination of surgery with subsequent chemotherapy may result in long-term patient survival. [19] The case by Matthias et al. [5] did not recur after three years of postoperative follow-up. The patient reported by Lam et al. [7] died 30 days postoperatively as a result of sepsis, and that by Couldwell et al. [6] died seven months after surgery as a result of tumor progression. Cases reported by Turner and Craig [8] and by Sela Bar G et al. [10] described a long term follow-up of two years and three years respectively. The other follow-up periods reported were seven months [9] and eight months. [2] The case reported by Dagcinar et al. [11] was in an eight-year-old boy, which recurred six and 12 months after surgery. This was a totally intraaxial tumor located in the sylvian fissure. From the analysis of the other seven case reports of POS, the following conclusions may be derived: 1) No sex preponderance (M:F = 1:1) 2) The mean age of presentation was 32.33 years (skewed because of a single pediatric case and the median age was 54.5 years representing a disease of middle age. 3) Dural based POS have a better prognosis as compared to intra-axial POS. 4) Adjuvant therapy for POS is controversial and no curative role may be ascribed to either chemotherapy or radiotherapy. In the present case, the patient fit the age profile and had no radiological recurrence at one and half year follow-up, corroborating the better prognosis of dural based primary osteosarcoma. She did receive a course of external beam radiation and chemotherapy. To the best of our knowledge, this is only the eighth case of dural based primary extraskeletal osteosarcoma. References
Copyright 2010 - Neurology India The following images related to this document are available:Photo images[ni10029f3.jpg] [ni10029f1.jpg] [ni10029f2.jpg] [ni10029t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}