 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 58, No. 1, January-February, 2010, pp. 131-134 Case Report Infectious intracranial aneurysm: Endovascular treatment with Onyx case report and review of the literature Pei Chao Zhao, Jin Li, Min He, Chao You Department of Neurosurgery, West China Hospital, Sichuan University, 37 Guo Xue Xiang Street, Chengdu, Sichuan - 610 041, China Correspondence Address: Dr. Chao You, Department of Neurosurgery,West China Hospital, Sichuan University, 37 Guo Xue Xiang Street, Chengdu, Sichuan - 610 041, China, zhpeichao@yahoo.com.cn Date of Acceptance: 15-Oct-2009
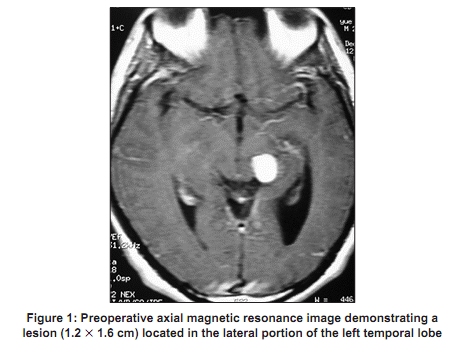
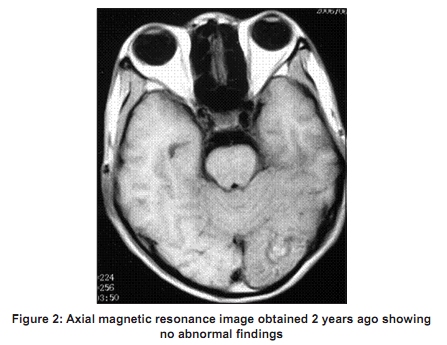
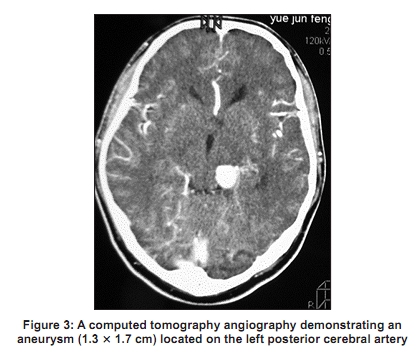
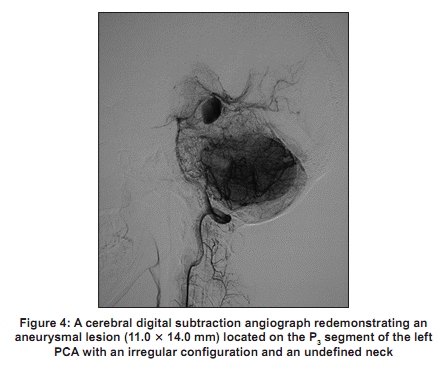
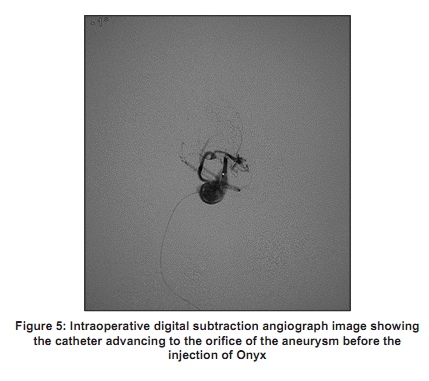
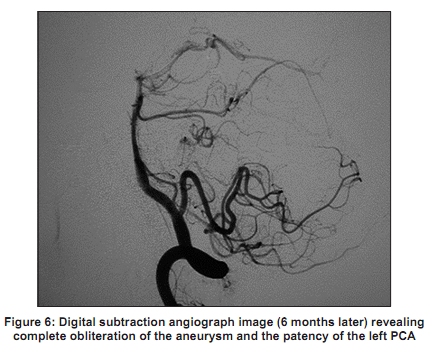
Code Number: ni10030 DOI: 10.4103/0028-3886.60429 Abstract Intracranial infectious (mycotic) aneurysms are very rare, but continue to be challenging and technically demanding, which need careful diagnosis and therapy. We present an 18-year-old man with an intracranial infectious aneurysm located on the left posterior cerebral artery who was successfully treated with endovascular embolization by a liquid embolic agent (Onyx) and who recovered well.Keywords: Endovascular treatment, infectious intracranial aneurysms, Onyx Introduction Intracranial infectious aneurysms (IIAs) are rare vascular lesions and are mainly located on the middle cerebral artery or its distal branches in up to 70% of the cases, less commonly on the anterior or posterior cerebral arteries. [1],[2],[3] Multiple treatment modalities currently available for these patients include medical, surgical and endovascular. Occlusion of the IIAs can be achieved either by surgery or, more recently, by endovascular treatment. [1],[3],[4] We report an IIA successfully occluded by endovascular treatment with Onyx. Case Report A 18-year-old male with a history of mitral valve replacement 2 years before presented to a local hospital with low-grade fever and malaise. He was initially diagnosed and treated as a case of common cold. One week later, he developed high-grade fever and chest discomfort and was transferred to our hospital. An echocardiogram revealed no vegetation and blood cultures grew methicillin-sensitive Staphylococcus aureus. Diagnosis of infectious endocarditis (IE) was considered and he was treated with high-dose nafcillin and levofloxacin. After 3 weeks of medical treatment, the patient had a sudden onset of seizure with transient loss of consciousness. Magnetic resonance image (MRI) of the brain demonstrated a lesion (1.2 x 1.6 cm) in the lateral portion of the left temporal lobe [Figure - 1] whereas an MRI obtained 2 years ago showed no lesion [Figure - 2]. Considering the possibility of infectious aneurysm, a subsequent computed tomography angiography (CTA) was performed, which demonstrated an aneurysm (1.3 x 1.7 cm) located on the left posterior cerebral artery (PCA) [Figure - 3]. He was then transferred to our department for further treatment. On examination he was normothermic, conscious and complained of headache. Neurological examination revealed no deficits. Laboratory examination showed a peripheral leukocyte count of 17 x 10 9 /L and blood and cerebrospinal fluid cultures were negative. Cerebral digital subtraction angiograph (DSA) demonstrated an aneurysm (11.0 x 14.0 mm) located on the P 3 segment of the left PCA [Figure - 4] with irregular morphology and an undefined neck. He was continued on antibiotic treatment with serial follow-up angiographic imaging. Follow-up CTA done at 2 weeks showed no change in the size of the aneurysm. At this stage endovascular embolization therapy was planned and patient was explained the risks and details of the procedure and an informed consent was taken. The procedure was performed under local anesthesia. The patient underwent anticoagulation with intravenous heparin to obtain an activated partial thromboplastin time two to three times the baseline value. With standard transfemoral approach, a 6F guilding catheter was advanced into the left vertebral artery with continuous flushing with normal saline. The catheter was superselectively advanced to the orifice of the aneurysm and Onyx-18 was injected into the lumen of the aneurysm [Figure - 5]. Imaging at the end of the procedure showed complete occlusion of the aneurysm and the patency of the parent artery was well preserved. The entire process was uneventful. The DSA performed 6 months after the embolization revealed complete obliteration of the aneurysm and the left PCA was still patent without any vascular complication [Figure - 6]. Discussion Intracranial infectious aneurysm was first reported by Church [5] in 1876 and account for 0.7-5.4% of all intracranial aneurysms. [1],[6] The causes of IIAs may be a systemic infections like infective endocarditis, local infections such as meningitis, cavernous sinus infection, orbital cellulitis and rarely, cryptogenic. [1],[3] The most common cause of IIAs is IE. Clinically significant IIAs in 2-10% of patients with IE. [7] Patients with prosthetic valve IE have a higher risk of developing IIAs when compared to patients with native valve IE. [8] Patients with IIAs have a distinct clinical profile when compared to patients with congenital intracranial aneurysms. In most patients with IIA the initial presentation is fever and later in the course they develop focal deficit or SAH. A pragmatic approach for the diagnosis of IIAs would be the use a combination of (1) clinical presentation; (2) characteristics of angiogram: Location on the distal cerebral arteries, changes in the size or morphology of the aneurysm on serial angiographies; and (3) identification of source of infection by appropriate investigations. The first step in the management of IIAs is medical, consisting of long-term antibiotic therapy. However, surgery may be indicated in patients with intracerebral haematoma with significant mass effect. [3],[4],[9] To determine the effectiveness of medical therapy, serial follow-up angiographic studies are necessary. The evolution of IIAs with antibiotic therapy is unpredictable, they may regress, disappear, persist, enlarge or rupture. [3],[4],[10] Response to antibiotic therapy is indicated by regression in the size of the aneurysm or complete resolution of the aneurysm. [10] However, the risk of rupture does not reduce with medical treatment. [1],[3] The low risk of IIAs rupture is less than 2%, however, the is associated with high morbidity and mortality approached 80%. [4],[11] It is thus prudent to have an aggressive therapeutic approach while dealing with IIAs. Surgical treatment plays an important role in the treatment of IIAs. [1],[8] The potential problems associated with surgery include risk of intraoperative rupture and clip erosion of the parent artery. These potential complications have been attributed to the irregular, fusiform morphology of the aneurysm and the acute inflamed, friable vessel wall. [3],[8],[9],[12] Delayed surgery after medical treatment allows the aneurysm to mature from a friable, acute lesion to a more fibrotic, subacute or chronic lesion, which make the aneurysm more amenable for direct clipping. [3] Even then, the high risk limits the use of surgical treatment. In fact, in some institutes, endovascular treatment is the treatment of first choice for patients with IIAs and is reserved for (1) enlarging IIAs while on antibiotic treatment, (2) persistent IIAs on the completion of antibiotic treatment and (3) stable ruptured IIAs with no elevated intracranial pressure and intracerebral hematoma. [3],[4],[12],[13],[14] However, surgical treatment still has a prominent role in patients with hematoma with mass effect or elevated intracranial pressure and when the infectious aneurysm is located on the most distal branches, which cannot be addressed for endovascular treatment. Most of the endovascular procedures can be adapted for most infectious aneurysms. Recently, Onyx (ethylene-vingl alcohol copolymer), a newer, nonabsorbable, nonadhesive liquid embolic material, has been used for the embolization of arteriovenous malformations. [15] To our knowledge, only two cases of IIAs treated with Onyx have been reported. [7] In our patient, the aneurysm had an irregular configuration and an undefined neck. Considering the potential risk of intra-procedure rupture of IIA by the coils, we chose the liquid embolic agent (Onyx-18) to occlude the aneurysm. The procedure was successful, the aneurysm was completely obliterated and the patency of PCA was preserved. It is suggested that endovascular embolization with Onyx-18 for IIAs is a safe and effective method, but the long-term efficacy needs further follow-up. References
Copyright 2010 - Neurology India The following images related to this document are available:Photo images[ni10030f3.jpg] [ni10030f1.jpg] [ni10030f2.jpg] [ni10030f6.jpg] [ni10030f5.jpg] [ni10030f4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}