 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 58, No. 1, January-February, 2010, pp. 137-139 Letter To Editor Coil Embolization of a ruptured anterior communicating aneurysm in Takayasu's arteritis Boby Varkey Maramattom Lourdes Heart Institute and Neuro Centre, Kochi, Kerala, India. Correspondence Address: Lourdes Heart Institute and Neuro Centre, Kochi, Kerala, India, bobvarkey@gmail.com Date of Acceptance: 06-Oct-2009
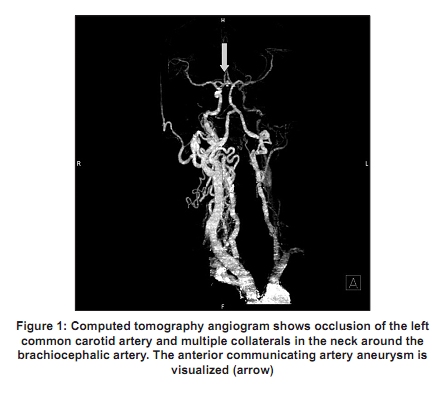
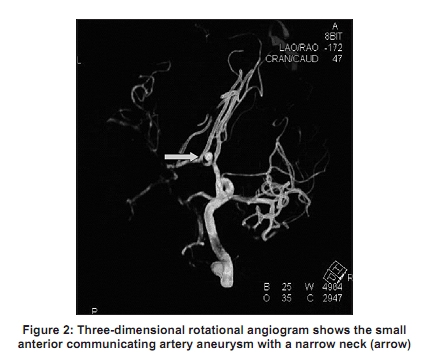
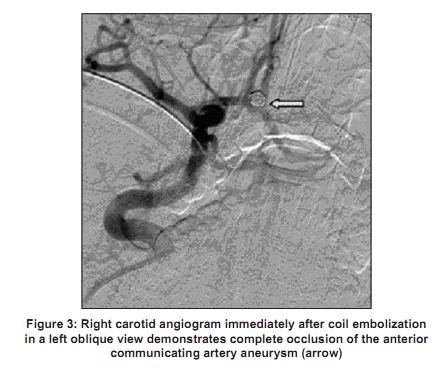
Code Number: ni10033 DOI: 10.4103/0028-3886.60404 Sir Takayasu′s Arteritis (TA), a rare type of vasculitis affects predominantly young females and involves the aorta and its large branches and the pulmonary arteries. It is more commonly reported from Japan, India and Mexico. [1] The arterial pathology is of three types: Stenotic, occlusive and aneurysmal, in descending frequency. Cerebral aneurysm and subarchnoid hemorrhage (SAH) is an exceedingly uncommon presentation of TA and only 20 odd cases have been reported in the literature. Coil embolization of cerebral aneurysm in TA have been reported earlier only on two occasions. [2],[3] However, ischemic events are more common and occur in 20-60% of patients and are related to stenosis and occlusion of the arch vessels. [4],[5] TA is classified into four angiographic types and in 1994, this classification was broadened to distinguish between the presence or absence of coronary (C+/C-) and pulmonary (P+P-) involvement. [6] We report successful coil embolization of a cerebral aneurysm in a patient with TA. A 29-year-old man presented with sudden severe headache. He had a past history of exertional angina at the age of 14 years. On evaluation, he was found to have aorto-arteritis (TA), with ostial stenosis of the right coronary and left mainstem arteries and had undergone a coronary bypass grafting for the same. He had subsequently been asymptomatic. On neurological examination at this admission he was slightly drowsy, but had no focal deficits. Ocular fundi were normal. Both the radial pulses were absent and a bruit could be heard on both the carotids. Abdominal examination revealed bilateral renal bruits. Blood pressure (BP) in the lower limbs was 210/90 mmHg and in the upper limbs it was 90/60 mmHg. Computerized tomography (CT) of the brain showed extensive SAH and mild hydrocephalus. CT angiogram showed a 4 x 5 mm anterior communicating artery (AcomA) aneurysm with a 2 mm neck and occlusion left common carotid artery (CCA) at its origin. The right CCA was enlarged and the right internal carotid artery (ICA) showed cross-circulation across the AcomA to the left hemisphere [Figure - 1]. There were numerous collateral vessels arising from the right common carotid artery. Within 12 h, the patient became drowsier and reaction of both the pupils to light was sluggish. A repeat CT brain showed increase in the size of the hydrocephalus. He had an external ventricular drain. Digitial substraction angiography (DSA) was performed the next day. Five thousand units of IV heparin was administered at the start of the procedure. After navigating a diagnostic catheter into the right CCA, the diagnostic catheter was exchanged for a 6 French guiding catheter, which was navigated up to the laceral segment of the right ICA. A 3D rotational angiogram revealed an AcomA aneurysm measuring 4.3 x 4 mm with a neck of 1.78 mm pointing anteriorly [Figure - 2]. A microcatheter and a microwire were then navigated through the ICA across the AcomA into the contralateral A1. After crossing the aneurysm, the microcatheter and microwire were brought back and hooked into the aneurysm. The microwire was then withdrawn and the aneurysm was packed with four detachable platinum coils (3 mm x 8 cm 3 D Axium, 2 mm x 3 cm Axium, 3 mm x 4 cm Axium and 3 mm x 6 cm Axium, ev3, Endovascular Inc.)[Figure - 3]. Postprocedure, aspirin was started at a dose of 325 mg/day. The patient was extubated after 36 h. He had Severe hypertension and as the BP could not be controlled by IV labetolol and enalapril he was started on IV nitroglycerin infusion. The pressures continued to be high, a systolic BP of 210 mmHg with a maximum dose of 200 mcg/h of IV nitroglycerin. On day 4, he developed dyspnea, oxygen desaturation and basal crepitations. A chest X-ray revealed bat-wing infiltrates suggestive of acute pulmonary edema. He was started on an infusion of torsemide 10 mg/h for 5 h and sodium nitroprusside. He was also started on oral amlodipine, losartan, moxonidine and alfa-methyldopa to control the BP. A subsequent renal artery Doppler was within normal limits. He was discharged 1 month later without any focal neurological deficits. This patient was noteworthy for a few reasons. Our patient is the third report of endovascular coiling of a cerebral aneurysm in TA. Importantly, neurointerventional procedures in patients with TA have to be modified as vascular access may be restricted. In this patient, there was only a single access through the right CCA, which supplied the entire anterior circulation. The right CCA was hyperplastic and extremely pulsatile. Moreover, the artery had become tortuous and dilated. Hence, the standard 100 cm guiding catheter could barely reach the petrous segment of the right ICA. This provided less stability during subsequent microcatheter manipulation into the distal ICA. It is also likely that occlusion of the contralateral ICA, cross-circulation from the right ACA and hyperdynamic flow through the AcomA might have predisposed to the formation of the Acom aneurysm. The postprocedure course of the patient was very labile and marked by hypertensive emergency, leading to left ventricular failure and pulmonary edema. This patient required as many as nine antihypertensive medications to control his blood pressure. In conclusion, this case highlights some of the challenges associated with the management of cerebral aneurysms in patients with TA. References
Copyright 2010 - Neurology India The following images related to this document are available:Photo images[ni10033f1.jpg] [ni10033f3.jpg] [ni10033f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}