 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 58, No. 1, January-February, 2010, pp. 139-141 Letter To Editor Fatal course of cerebral vasculitis induced by neuroborreliosis Fredrik Buchwald1 , Kasim Abul-Kasim2 , Johan Tham3 , Bjarne U. Hansen4 1 Departments of Neurology, 2 Radiology, 3 Infectious Diseases and 4 Rheumatology, Faculty of Medicine, University of Lund, Malmö University Hospital, Malmö, Sweden. Correspondence Address: Fredrik Buchwald, Department of Neurology, Faculty of Medicine, University of Lund, Malmö University Hospital, Malmö, Sweden, fredrik.buchwald@skane.se Date of Acceptance: 12-Oct-2009
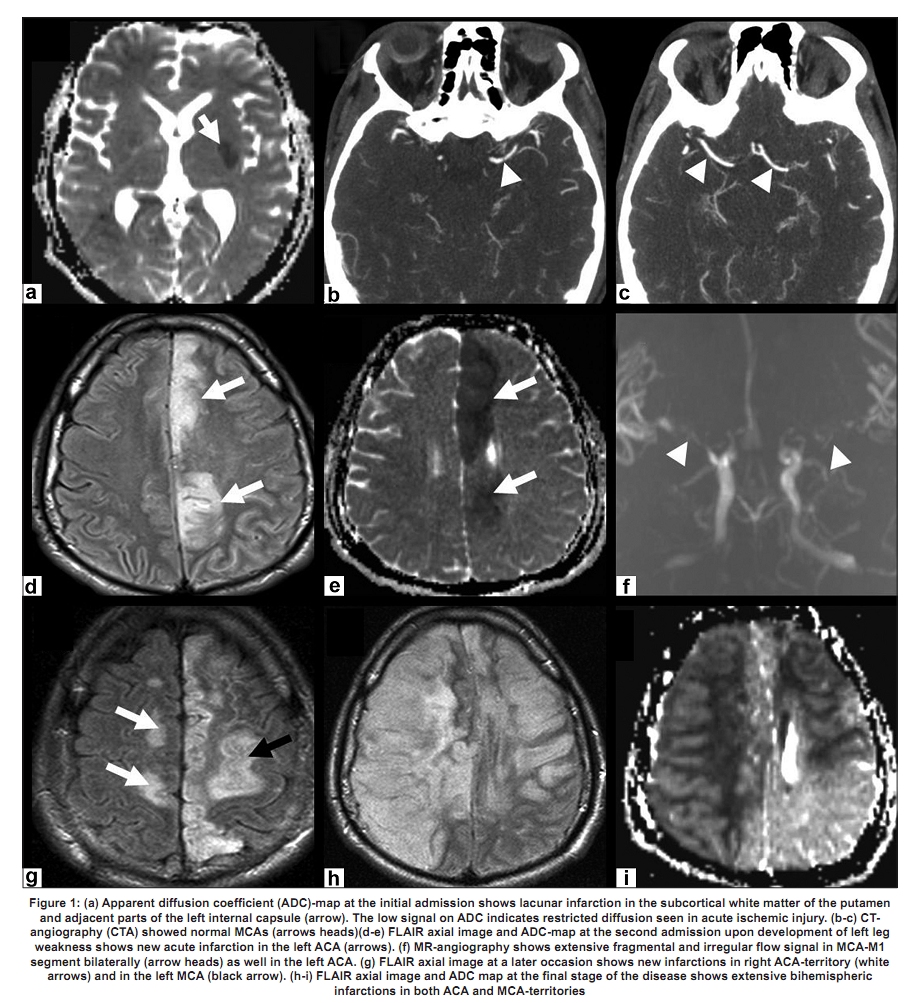
Code Number: ni10034 DOI: 10.4103/0028-3886.60407 Sir, Borreliosis is a tick-borne illness caused by the spirochete Borrelia and the different causative strains identified include B. burgdorferi sensu strictu in America and B. garinii and B. afzelii in Europe. Clinical manifestations are wide and vary in severity. The disease is divided into three stages: 1) early localized disease characterized by skin lesions (erythema migrans); 2) early disseminated disease characterized by neurologic and/or cardiac involvement; and 3) late disease characterized by arthritis and/or rare neurologic complications. [1],[2] Cerebral vasculitis is a very rare, usually a nonfatal complication. [3],[4],[5] A fatal case of neuroborreliosis complicated by cerebral vasculitis in a young male patient prompted us to present this case. In May 2008 a 25-year-old male smoker presented with a sudden onset of right-sided hemiparesis and at admission he had partially recovered. Computerized tomography (CT) scan and magnetic resonance imaging (MRI) revealed a small left subcortical infarction. Angiographic sequences, both CT-angiography and MR-angiography, were essentially normal [Figure - 1] a-c. Diagnostic work-up for vascular risk factors was normal. During springtime he had been bitten by a tick but as he had no erythema, headache, fever or other alarming symtoms the possibility of neuroborreliosis was excluded. He was put on aspirin 160 mg once a day and dipyridamole 200 mg twice a day. His state continued to improve and one week later he was discharged. About five weeks after discharge, his condition slowly worsened. His original symptoms progressed in severity and, in addition, he developed dysphasia and paresis of his left leg. He returned to our emergency room about 3 weeks later and a repeat neuroradiological investigation with MRI and CT, including angiographic sequences, showed an infarction in the territory of the left anterior cerebral artery (ACA) and extensive changes in the calibre of basilar artery, both middle cerebral arteries (MCA) and left ACA, the latter being occluded. These features were consistent with cerebral vasculitis [Figure - 1] d-f. Cerebrospinal fluid (CSF) examination revealed elevated protein (1.88 g/l) and increased white blood cells (monocytes 6.3 x 106/l). CSF was positive for specific borrelia IgM-antibodies (1.35 ELISA index pos) and serum borrelia IgG-antibodies titers were elevated. These findings were strongly suggestive of neuroborreliosis, even though the CSF polymerase chain reaction (PCR) showed no borrelia-DNA. Extensive radiological and laboratory work-up for systemic vasculitis and connective tissue diseases was negative. Work-up for other infectious diseases was also negative. He was treated with oral doxycycline 200 mg twice daily for 12 days. His vasculitis was initially treated with IV methylprednisolone 1 g for three consecutive days followed by oral prednisone 60 mg per day. In spite of this treatment, his state continued to deteriorate. Repeat MRI including angiographic sequences showed progression of cerebral vasculitic changes and more ischemic areas [Figure - 1]g. Repeat CSF examination after antibiotic treatment revealed normal levels of specific borrelia IgM-antibodies. He was further treated with IV cyclophosphamid, 15 mg/kg every second week. Three weeks later he developed brain edema due to extensive bihemispheric infarctions [Figure - 1]h-i and died of transtentorial and subfalcine herniation. With respect to his family′s wish, an autopsy was not performed. Probably this is the only reported case of fatal cerebral vasculitis due to neuroborreliosis. The diagnosis of cerebral vasculitis was based on clinical course, CSF findings, MRI and CT/MR-angiographic findings even though conventional cerebral angiography and histopathological confirmation were not performed in this patient. [6],[7] Elevated titers of specific borrelia IgM-antibodies in the CSF suggest that the cerebral vasculitis in this patient probably was a complication of neuroborreliosis. [3],[4],[5] The absence of a preceding erythema migrans is not unusual, [1],[2],[8] however, total absence of other symptoms and signs of borreliosis as seen in this patient is rare. The histopathological substrate for neuroborreliosis is assumed to be an angiopathy of small vessels with mononuclear perivascular infiltration. Cerebral vasculitis in neuroborreliosis is rare and the pathogenesis of the angiopathy is uncertain. [9] Cerebral vasculitis in neuroborreliosis improves in som patients with specific antibiotic treatment [3],[4],[5],[9] thus suggesting that cerebral vasculitis in neuroborreliosis may be due to direct angio-invasion by the spirochetes. In patients who fail to respond to specific antibiotics, immunosuppressive treatment may be necessary [6] thus suggesting immune-mediated mechanisms. In our patient CSF specific borrelia-IgM-antibodies returned to normal levels after adequate antibiotic treatment [10] while vasculitic changes progressed, thus supporting the latter theory. In our patient delayed institution of appropriate specific treatment might have resulted in the fatal outcome. A contributing factor was failure on the part of the patient by not calling on us in spite of three weeks of deterioration. This case illustrates the importance of having an index of suspicion of borrelia infection, especially in high-endemic areas such as southern Sweden, [2] both when dealing with "cryptogenic" stroke and cerebral vasculitits. References
Copyright 2010 - Neurology India The following images related to this document are available:Photo images[ni10034f1.jpg] |
| |||||||||

{kind=link}