 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 58, No. 1, January-February, 2010, pp. 141-144 Letter To Editor Facio-auriculo-vertebro-cephalic spectrum of Goldenhar syndrome Amit Mahore, Nitin Dange, Santhosh Nama, Atul Goel Department of Neurosurgery, Seth Gordhandas Sunderdas Medical College and King Edward VII Memorial Hospital, Parel, Mumbai, India. Correspondence Address: Amit Mahore, Department of Neurosurgery, Seth Gordhandas Sunderdas Medical College and King Edward VII Memorial Hospital, Parel, Mumbai, India, amit2mahore@yahoo.co.in Date of Acceptance: 08-Oct-2009
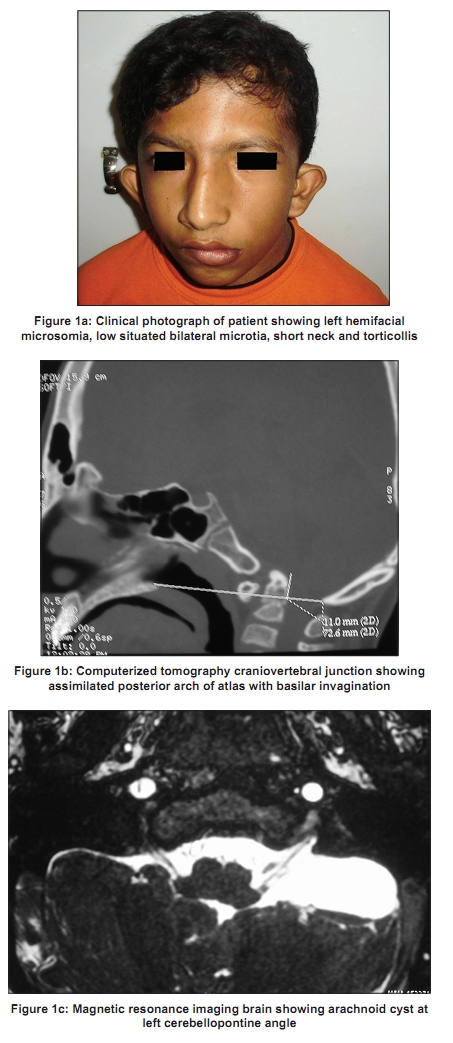
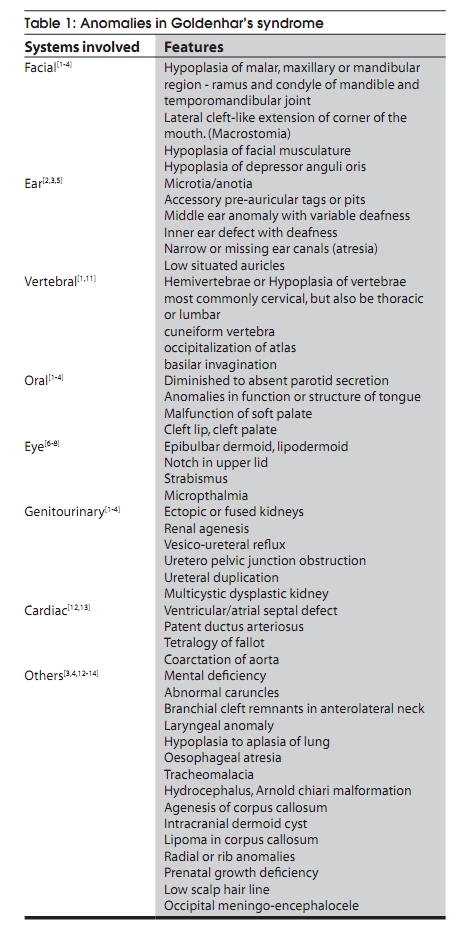
Code Number: ni10035 DOI: 10.4103/0028-3886.60409 Sir, A 12-year-old male child, born of a non-consanguineous marriage, was referred for evaluation of a recent onset episode of generalized tonic clonic seizure. Antenatal and intranatal periods were uneventful. Patient was operated for an occipital meningocele and a tag with cleft at right cheek thirteen days after birth by a pediatric surgeon. Patient had bilateral deafness since birth. Physical examination of the child showed left lower motor neuron facial paresis, bilateral microtia and inferiorly situated ears. In addition, he had scars of previous surgeries, short neck; torticollis and left hemi-facial hypoplasia [Figure - 1]a. Patient did not have any other deficits. Reflexes were normal. Echocardiogram was normal. Ultra sonography of abdomen revealed crossed ectopic kidneys. Computerized tomography (CT) scan and X-ray of craniovertebral junction and cervical spine revealed assimilation of posterior arch of atlas with basilar invagination [Figure - 1]b. Magnetic resonance imaging (MRI) revealed an arachnoid cyst in the left cerebello-pontine angle [Figure - 1]c. CT-scan of the temporal bone showed sclerosis of middle and inner ear bilaterally. Audiogram report showed bilateral severe sensorineural hearing loss in both the ears. Diagnosis of facio-auriculo-vertebral dysplasia or Goldenhar′s syndrome was made. Patient′s relatives did not give consent for any operative intervention. Patient was advised antiepileptic drug and close follow-up. There was no family history suggestive of this syndrome in the patient′s family. Parents and other siblings of patient were normal. Patient was intellectually normal. The patient is a successful student of school for deaf and mute. Franceschetti-Goldenhar syndrome or Goldenhar-Gorlin syndrome, also known as facioauriculovertebral spectrum (FAV), first and second branchial arch syndrome, or oculo-auriculovertebral (OAV) spectrum, is associated with various abnormalities. Different combinations of clinical anomalies associated with this syndrome have been given different names. [1],[2],[3],[4] The syndrome was first recorded by German physician Carl Ferdinand Von Arlt in 1845, and Goldenhar in 1952 defined the syndrome more clearly. [1],[2],[3],[4] Conductive and/or sensorineural hearing loss is present in 50% of the patients with this syndrome. [5] The etiology of the hearing loss is varied and may include missing or malformed outer ear (anotia and microtia), narrow or missing ear canals (atresia), abnormal skin cartilage on or in front of the ears (preauricular tags) and abnormalities in the middle or inner ear. It is a very rare kind of syndromic deafness with an incidence of 1 per 3500 to 5000 live births. [1],[2],[3],[4],[5] It is present in 1 in 1000 children with congenital deafness. The male to female ratio of this syndrome is 3:2. Although most cases are sporadic, families manifesting autosomal dominant and recessive traits have been described, with evidence that the latter is more frequently characterized by eye abnormalities. [5],[6],[7],[8],[9],[ 10] A small percentage also has mental retardation associated with this syndrome. Epibulbar dermoids and lipodermoids, coloboma of the eyelid, microphthalmia, strabismus and retinal anomalies are the associated ocular problems in Goldenhar syndrome. [7],[8],[9],[10] Our patient had most of the features of FAV syndrome except the eye anomalies associated with this syndrome [Table - 1]. However, such a combination of FAVsyndrome with basilar invagination, occipital meningocele and arachnoid cyst in posterior fossa has not been reported. Vertebral anomalies have been shown in 40 to 60% of cases diagnosed as Goldenhar syndrome. Failure of segmentation is the most common abnormality present in the neck region, and failure of formation most frequently occurs in the upper thoracic spine. Hemivertebra, cuneiform vertebra and occipitalization of atlas are most commonly seen. [11] Congenital heart diseases are seen in 40 to 60% of patients with Goldenhar′s syndrome, especially VSD, ASD, patent ductus arteriosus (PDA), tetralogy of Fallot and coarctation of the aorta. [12],[13] A high incidence of structural and functional abnormalities of the pharynx and larynx has been found associated with this syndrome, and these anomalies may contribute to an increased risk of airway obstruction, communication impairment and morbidity. [3],[4],[12],[13] The etiology is not known, but is thought to be due to exposure to viruses or chemicals during pregnancy, due to abnormal vascular supply to the first and second arch and abnormality of mesoblastic development affecting the formation of vertebral and branchial systems. Some researchers suggest that the disorder may be due to interaction of many genes with environmental factors (multifactorial inheritance). Expression of MSX class genes permit clear understanding of the variability and different degrees of severity of the anomalies of OAV spectrum. The MSX homeobox genes also play a crucial role in the differentiation of first branchial arch. [6],[7] In many cases, this syndrome goes unnoticed in Indian population due to the lack of knowledge about its features. Prognosis is good in the absence of mental retardation and cardiac anomalies. The neurosurgical problems are also amenable to surgical corrections like the structural anomalies of the heart, eyes, ears, jaw and teeth in Goldenhar′s syndrome.[14] References
Copyright 2010 - Neurology India The following images related to this document are available:Photo images[ni10035t1.jpg] [ni10035f1.jpg] |
| |||||||||

{kind=link}
{kind=link}