 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 58, No. 1, January-February, 2010, pp. 152-154 Letter To Editor Contrecoup epidural hematoma: Case report and review of literature Satoru Takeuchi, Yoshio Takasato, Hiroyuki Masaoka, Naoki Otani Department of Neurosurgery, National Hospital Organization Disaster Medical Center, Japan. Correspondence Address: Satoru Takeuchi, Department of Neurosurgery, National Hospital Organization Disaster Medical Center, Japan, s.takeuchi@room.ocn.ne.jp Date of Acceptance: 23-Oct-2009
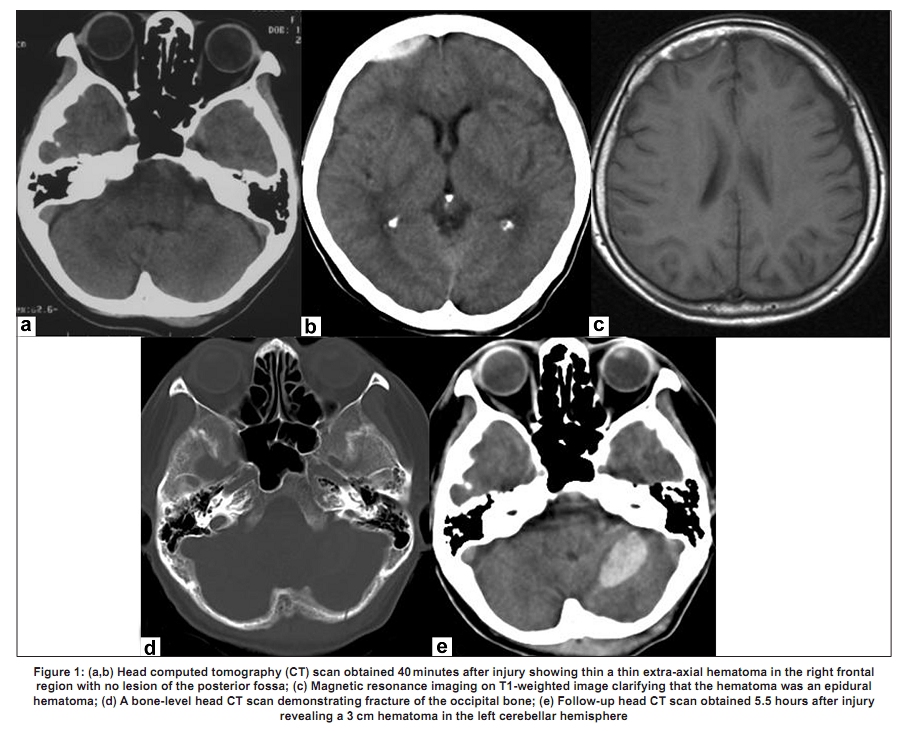
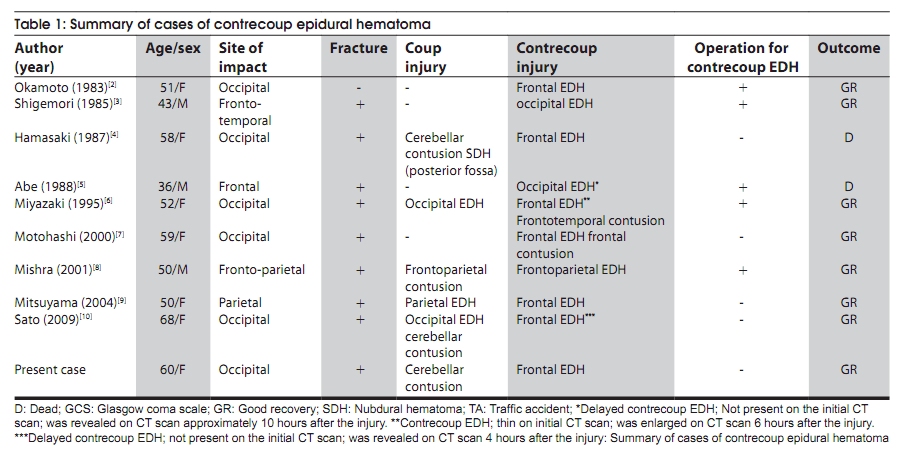
Code Number: ni10042 DOI: 10.4103/0028-3886.60425 Sir, A 60-year-old female was struck by a slow-moving vehicle which hit her occiput. On admission, her blood pressure was 128/75 mm Hg. Neurological examination was normal. A head computed tomography (CT) scan obtained 40 minutes after injury showed a thin, extra-axial hematoma in the right frontal region, with no lesion of the posterior fossa [Figure - 1]a and b. T1-weighted magnetic resonance images (MRI) confirmed that the hematoma was an epidural hematoma (EDH) [Figure - 1]c. A bone-window head CT scan revealed fracture of the occipital bone [Figure - 1]d. A follow-up head CT scan obtained 5.5 h after injury revealed a 3-cm hematoma in the left cerebellar hemisphere [Figure - 1]e. There was no evidence of a concurrent blow in the frontal region. The patient was treated conservatively and the hematoma showed no remarkable change in size. The patient was discharged 12 days after the injury with no neurological deficits. EDHs commonly result from coup head injuries. [1] However, contrecoup EDH cases are rare, and only nine cases have been reported in the literature. [2],[3],[4],[5],[6],[7],[8],[9],[10] The clinicoradiological features of all the ten cases including the present case are summarized in [Table - 1]. The interesting features of patients with contrecoup EDH included: Female predominance, relatively old mean age, high frequency of frontal region involvement, and high rates of delayed appearance of EDH. In contrast, cases of EDH are generally more frequent among males, with a Male:Female ratio of 4:1. The peak incidence of EDH is in the second decade, with a mean age of 20-30 years; EDH is rare in patients older than 50-60 years. [1] The female predominance and older age of the patients identified in our literature review suggests that contrecoup EDH is a different entity from common EDH. EDH is most frequently located in the temporoparietal and temporal regions, [1] while contrecoup EDH is most frequently located in the frontal regions (70%). This could be explained by the fact that the dura mater of the lateral frontal region is easily detached from the inner table, as found during craniotomy procedures. [9] Delayed EDH is considered uncommon, with a reported incidence of approximately 3%. In contrast, delayed contrecoup EDH was observed in two patients in this study (20%). This suggests that repeat CT imaging is necessary, especially between 4-10 hours after injury. The mechanism of contrecoup EDH remains unclear. Surgery for contrecoup EDH has revealed no damage to the larger arteries, though oozing from small dural vessels was recognized in one case. [6] Dural separation and dural vessel injury caused by distortion of the cranium brought on by the force of impact are possible mechanisms that could contribute to the development of EDH. References
Copyright 2010 - Neurology India The following images related to this document are available:Photo images[ni10042t1.jpg] [ni10042f1.jpg] |
| |||||||||


{kind=link}
{kind=link}