 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 58, No. 1, January-February, 2010, pp. 154-155 Letter To Editor A rare case of metachronous double spinal dural arteriovenous fistula Amit Dagar, Manish K. Kasliwal, Ashish Suri, Subhash Kumar1 , Ajay Garg1 , Bhawani S. Sharma 1Department of Neurosurgery and Neuroradiology, Neurosciences Centre, All India Institute of Medical Sciences, New Delhi - 110 029, India. Correspondence Address: Department of Neurosurgery and Neuroradiology, Neurosciences Centre, All India Institute of Medical Sciences, New Delhi - 110 029, India, surineuro@hotmail.com Date of Acceptance: 23-Oct-2009
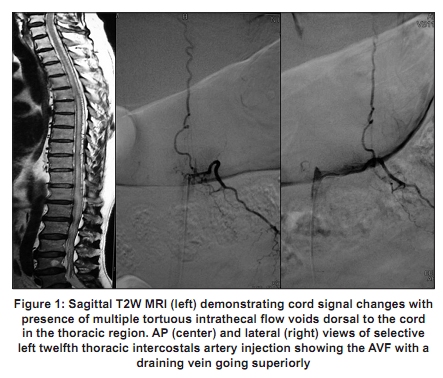
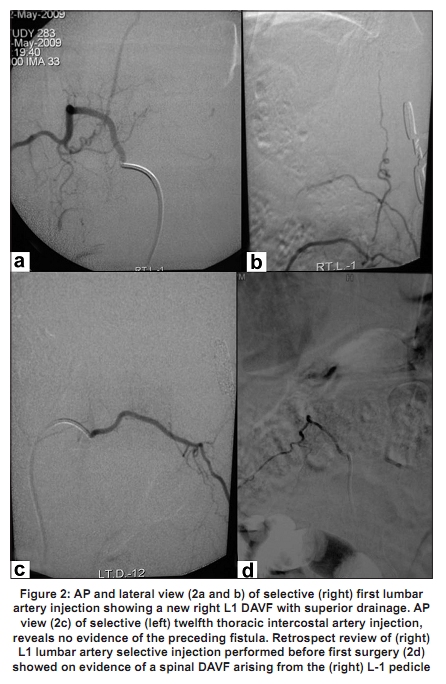
Code Number: ni10043 DOI: 10.4103/0028-3886.60427 Sir, Spinal dural arteriovenous fistulas (DAVFs), the most common of spinal vascular malformations consist of an AVF located in the dura mater of the nerve root and/or adjacent spinal dura and is most often, single. [1] Reports of multiple spinal DAVFs are rare; most of which presented synchronously. [2],[3],[4] True metachronous spinal DAVF is a very rare entity. [5] A 58-year-old male presented with gradual onset spastic paraparesis with bladder symptoms of one year duration. Magnetic resonance imaging (MRI) and spinal angiography revealed the presence of signal changes in the cord with a left T12 DAVF. [Figure - 1] Intraoperatively, there was a radicular feeding artery communicating with venous system at the dural sleeve with dilated coronal venous plexus which was coagulated and divided. Patients improved symptomatically gradually over six weeks following surgery and started to walk with support for two years when he again had deterioration in power with worsening of symptoms. Spinal angiogram revealed the presence of a newer DAVF at right L1 level with no evidence of previously treated DAVF at left T12 level. [Figure - 2] Previous spinal angiogram were reviewed to rule out preexistence of right L1 DAVF at the time of first spinal angiography, [Figure - 2] thus documenting the true development of a metachronous double spinal DAVF. The patient underwent surgery again for the second DAVF with some improvement at a three-month follow-up. Multiple spinal DAVFs are rare most of them reported were diagnosed either synchronously or were documented during second examination, being missed during the initial angiography. [2],[3],[4] Though the exact pathophysiology of DAVF remains unclear, late onset of symptoms, lack of other associated vascular anomalies, predominant occurrence in males and development of such lesions following trauma and following surgery strongly points towards an acquired etiology. [1],[2],[5] The development of metachronous double DAVF as described by us and Rizvi et al. [5] further adds support to an acquired origin of these vascular spinal lesions. Various hypotheses have been advocated in cases with multiple DAVF like thrombosis at several sites due to hypercoagulable state or venous stagnation and subsequent thrombosis due to one DAVF. [2],[3],[4],[5] Though the exact mechanism of development of metachronous DAVF as described in the present case remains controversial, chances of venous thrombosis occurring in the spinal/medullary veins or iatrogenic venous injury after surgical treatment of the original spinal DAVF appears to be the most probable etiology. Progressive pial venous thrombosis causing venous ischemia and subsequent spinal cord infarction can cause deterioration a few days after embolization; so can a development of irreversible ischemic damage to the spinal cord. [5],[6] Apart from this, development of a newer DAVF can also lead to failure of treatment with recurrence of symptoms as in the present case. This can also be due to the presence of another synchronous DAVF, which was missed on an initial angiogram as reported by some authors. [4] Though diagnosis of double or multiple metachronous spinal DAVF is rare, its clinical importance cannot be overemphasized as recognition of such cases is essential highlighting the need for careful and thorough performance of spinal angiography at all levels especially during follow up in cases with poor response to treatment. Magnetic resonance angiography (MRA) can also be a useful non invasive follow-up modality for these patients and can help rule out the development of a metachronous DAVF. The rare occurrence of metachronous double spinal DAVFs as shown in the present case should be considered a possibility accounting for delayed neurological deterioration following successful treatment and a complete spinal angiography at all levels/MRA should be performed to rule out this rare occurrence. References
Copyright 2010 - Neurology India The following images related to this document are available:Photo images[ni10043f2.jpg] [ni10043f1.jpg] |
| |||||||||

{kind=link}
{kind=link}