 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 58, No. 1, January-February, 2010, pp. 156-158 Letter To Editor Cerebrospinal fluid rhinorrhea and acquired anterior basal encephalocoele in a patient with colloid cyst of the third ventricle Kythasandra Shivakumar Deepak, Chandrasekharan Kesavadas, Tirur Raman Kapilamoorthy, Gireesh Menon1 Departments of Imaging Sciences and Interventional Radiology and 1 Neurosurgery, Sree Chitra Tirunal Institute for Medical Sciences and Technology, Trivandrum - 695 011, India. Correspondence Address: Chandrasekharan Kesavadas, Department of Imaging Sciences and Interventional Radiology, Sree Chitra Tirunal Institute for Medical Sciences and Technology, Trivandrum - 695 011, India, chandkesav@yahoo.com Date of Acceptance: 23-Oct-2009
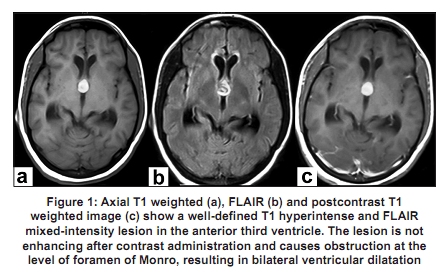
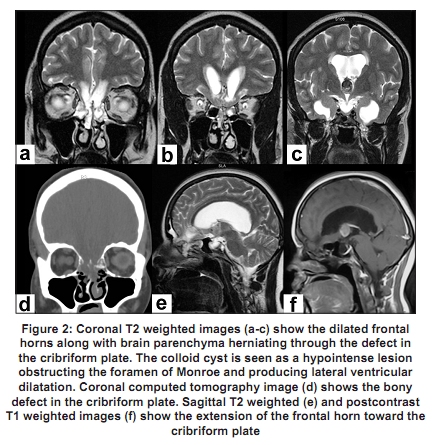
Code Number: ni10045 DOI: 10.4103/0028-3886.60431 Sir, Colloid cyst of the third ventricle is a well known cause for obstruction at the foramen of Monro with consequent dilatation of lateral ventricles. The lesion is often stable even though acute obstruction with coma and death has been reported. [1] Anterior basal encephalocele, usually due to a defect in the ethmoidal or sphenoidal bones, is congenital, traumatic or postoperative in origin. [2] Rarely, long-standing raised intracranial pressure can result in this condition. [3] The acquired variety is usually associated with defects in the vault or base of the skull. Patients with basal encephalocele can present with cerebrospinal fluid (CSF) rhinorrhea. [4] We describe a female patient presenting with episodic headache, seizures and CSF rhinorrhoea found to have on imaging evaluation a colloid cyst of the anterior third ventricle with anterior basal encephalocele. A 37-year-old female patient presented with complaints of recurrent episodes of bitemporal headache associated with vomiting since three years, memory disturbance since six months and seizures since four months. She also had a continuous leak of watery fluid from the left nostril since four months. She had no past history of head injury. On clinical examination her vitals were stable. She had bilateral anosmia and bilateral lateral rectus movement restriction. There was no other focal neurological deficit. The analysis of CSF showed mild lymphocytosis. Gram staining and culture of CSF were negative. Computed tomography (CT) of the brain showed a well-defined isodense lesion in the anterior third ventricle causing obstruction of CSF flow at the level of foramen of Monro. The lesion appeared hyperintense in T1 weighted sequence and mixed intensity in the fluid-attenuated inversion recovery sequence. There was no contrast enhancement [Figure - 1]. The lateral ventricles were dilated. The frontal horns of the lateral ventricles along with neighboring brain parenchyma were seen herniating through a bony defect in the cribriform plate [Figure - 2]. She underwent right precoronal parasagittal minicraniotomy, interhemispheric transcallosal approach and excision of colloid cyst. Histopathology of the lesion was consistent with the diagnosis of colloid cyst. Postoperatively, her CSF rhinorrhea stopped. On her first postsurgical follow-up hospital visit, she was doing fine. Colloid cyst usually presents in the 3 rd -4 th decade of life. The patient usually presents with headache. In most of the patients (90%) this lesion is stable; however, sudden enlargement with acute hydrocephalus resulting in coma/death is well documented. [1] Hydrocephalus can be intermittent or positional. Presentation as pseudoeclampsia and normal tension glaucoma has been reported. [5],[6] Our patient with long-standing episodic headache and recent-onset memory disturbance presented to our hospital with CSF rhinorrhea. A literature search revealed only one report of a patient with colloid cyst presenting with CSF rhinorrhea. [7] "Obstructive" rhinorrhea is the term used for CSF leakage that arises as the direct consequence of long-standing or intermittently severe hydrocephalus due to some lesion interrupting the flow of CSF. [7] This condition has been described with aqueduct stenosis and intracranial mass lesions obstructing the CSF flow. [7],[8],[9] Rovit et al. have termed such rhinorrhea as high-pressure CSF rhinorrhea. [7] The relatively static nature or extremely slow rate of growth of the obstructing lesion appears to be a factor in the eventual production of CSF fistula. A fistulous tract connecting the ventricular system with the paranasal sinuses usually develops in long-standing hydrocephalus. [7] Barazi et al., in a recent report, have termed this as pulsion diverticulum. [10] Our patient developed such a tract from the frontal horn of the lateral ventricle into the anterior basal encephalocele. It is well known that to accommodate increasing pressure within the intracranial cavity the brain parenchyma tries to move through the fissures and foramen. The cribriform plate of the ethmoid bone is a relatively weak bone perforated by multiple foramina for the passage of the olfactory nerves. [11] Long-standing elevated intracranial pressure can produce thinning of the floor of the anterior cranial fossa and eventual disruption of the cribriform plates. [3],[12] Our patient had probably developed a defect in the cribriform plate of ethmoid bone secondary to the pressure exerted by the chronic enlarged frontal horns of lateral ventricles. The enlarged frontal horns along with the fistulous tract could be responsible for the encephalocele. The CSF leakage in these patients usually ceases after removal of the obstructing lesion. [7] In few patients, the leakage is reduced to an occasional trickle. In our patient, the CSF rhinorrhea stopped completely after the removal of the colloid cyst and restitution of the patency of CSF pathway. References
Copyright 2010 - Neurology India The following images related to this document are available:Photo images[ni10045f2.jpg] [ni10045f1.jpg] |
| |||||||||

{kind=link}
{kind=link}