 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 58, No. 1, January-February, 2010, pp. 158-160 Letter To Editor Post Gamma knife subarachnoid hemorrhage and hydrocephalus Chandrasekharan Kesavadas, Biji Bahuleyan1 , Somenath Chatterjee, Tirur Raman Kapilamoorthy Departments of Imaging Sciences and Interventional Radiology and 1Neurosurgery, Sree Chitra Tirunal Institute for Medical Sciences and Technology, Trivandrum - 695 011, Kerala, India. Correspondence Address: Chandrasekharan Kesavadas, Department of Imaging Sciences and Interventional Radiology, Sree Chitra Tirunal Institute for Medical Sciences and Technology, Trivandrum - 695 011, Kerala, chandkesav@yahoo.com Date of Acceptance: 15-Oct-2009
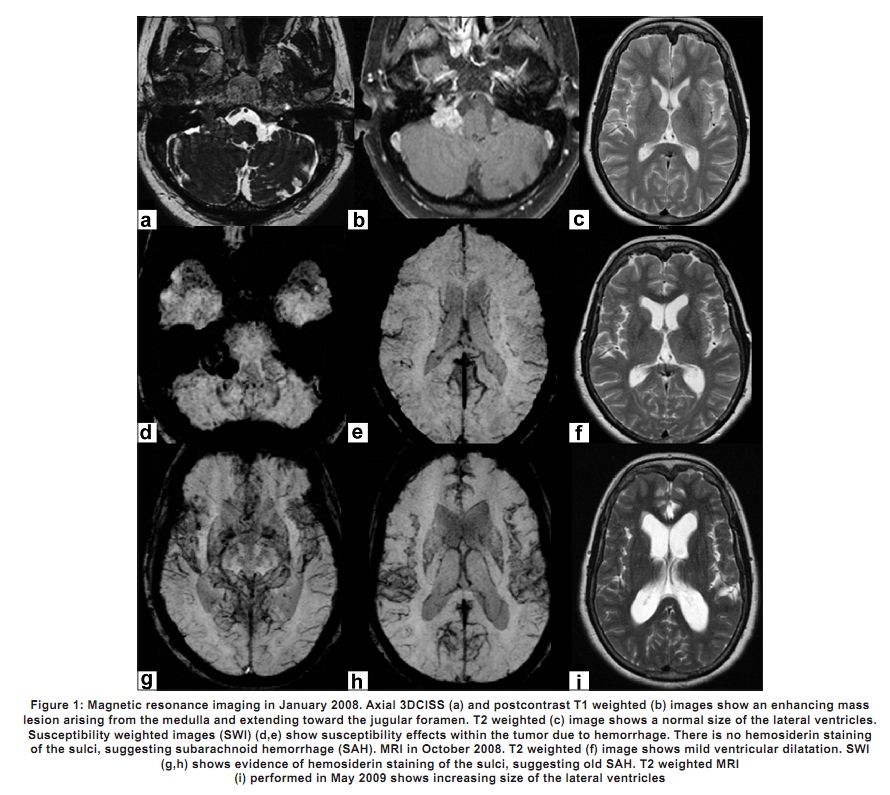
Code Number: ni10046 DOI: 10.4103/0028-3886.60432 Sir, A 60-year-old female presented with complaints of right-sided neck pain, right-sided hearing loss and gait unsteadiness for two months duration. The neurological examination showed right twelfth nerve palsy. Routine laboratory investigations, including bleeding parameters, were within normal limits. Magnetic resonance imaging (MRI) of the brain performed in January 2008 [Figure - 1]a- e revealed a well-defined, heterogeneous mass in the right jugular foramen extending into the right cerebello-pontine (CP)angle and the right internal auditory meatus, abutting the seventh and the eighth nerve complex. On susceptibility weighted images (SWI), the lesion showed areas of susceptibility, suggesting areas of bleed. The ventricular system appeared normal. A radiological diagnosis of lower cranial nerve schwannoma was considered. Because there was no significant blush in the digital subtraction angiogram, the possibility of glomus jugular tumor/hemangioma was ruled out. The intracranial vasculature did not reveal any aneurysm or vascular malformation. In view of the small size of the lesion,high risk of lower cranial nerve palsy and resultant morbidity after surgery, it was decided to refer the patient for gamma knife therapy. In February 2008, the patient underwent gamma knife therapy. The 7.7 cc of the tumor volume received 16 Gy to 50% isodose, 96% of the tumor received more than 16 Gy. 839.8 mm 3 of the brainstem received more than 10 Gy dose. After two weeks of the treatment, her right ear and neck pain subsided. In August, she had severe pain in the back of the head and neck that continued for the next two months. An MRI performed in October 2008 revealed subarachnoid hemorrhage (SAH) that was visualised in only the SWI. There was mild hydrocephalus [Figure - 1]f-h. Computed tomography (CT) head with CT angiography (performed on a 64-slice multidetector CT) could not detect SAH or intracranial aneurysm. The patient started developing progressive difficulty in walking in the next four to six months. A repeat MRI [Figure - 1]i in May 2009 showed increasing hydrocephalus, which needed shunting. The patient improved symptomatically after the shunting. Radiosurgical management of intracranial mass lesions can rarely lead to vascular complications, such as vessel occlusion or hemorrhage. [1] SAH is a less-reported complication following this form of therapy. There are few reports of patients who had rupture of the aneurysm that was probably induced by gamma knife surgery for schwannoma. [2],[3],[4] Our patient developed SAH and hydrocephalus, which were detected on imaging eight months after gamma knife irradiation. Unlike the previous cases that reported SAH secondary to aneurysm rupture, the patient described in this report did not reveal any aneurysm on CT angiography. There are few questions in this report that need discussion. Was the gamma knife therapy responsible for the SAH? In cases where the preradiation MRI shows evidence of microhemorrhages within the tumor, should the radiation dose be lesser? The SAH could very well have been due to the therapy. However, there are reports in the literature [5] and the authors have also seen cases where an acoustic schwannoma can present with SAH. These cases had no history of radiation. Hence, it can be argued that the SAH may be incidental and not related to the therapy. We also observed that the radiation dose given to our patient was on the higher side. This could probably be the reason for tumor capsule rupture and bleed. However, with a single case report, it is inappropriate to conclude that a higher radiation dose can result in bleed. This report highlights another important observation on the ability of SWI in picking up old SAH that is not seen in CT. But, for this sequence, the cause for the increasing ventricular dilatation could not have been diagnosed. Previous studies have suggested that proliferation of arachnoid cells and leptomeningeal fibrosis, triggered by an inflammatory reaction or blood clotting products, may impair cerebrospinal fluid flow through the arachnoid villi, resulting in hydrocephalus in patients with SAH. [6] References
Copyright 2010 - Neurology India The following images related to this document are available:Photo images[ni10046f1.jpg] |
| |||||||||

{kind=link}