 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 58, No. 1, January-February, 2010, pp. 160-162 Letter To Editor Melanotic craniopharyngioma, an unusual variant in a young female Nandita Ghosal, Ravi Dadlani 1 , Sai Kiran1 , A. S. Hegde2 Departments of Pathology and Transfusion Medicine, 1 Neurosurgery, 2 Neurosciences, SSSIHMS, Bangalore, India. Correspondence Address: Nandita Ghosal, Department of Pathology and Transfusion Medicine, SSSIHMS, Bangalore, India, nandita.g@rediffmail.com Date of Acceptance: 02-Nov-2009
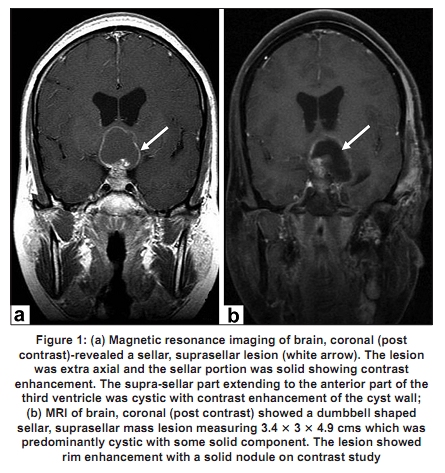
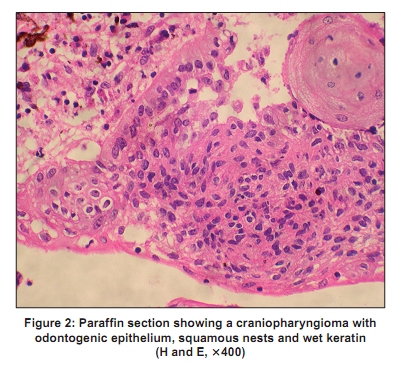
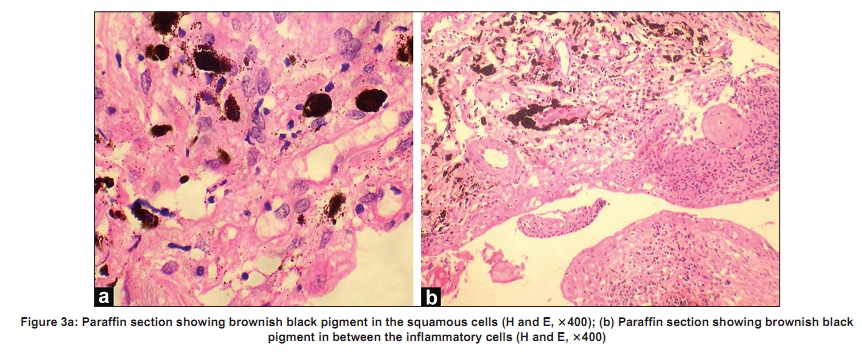
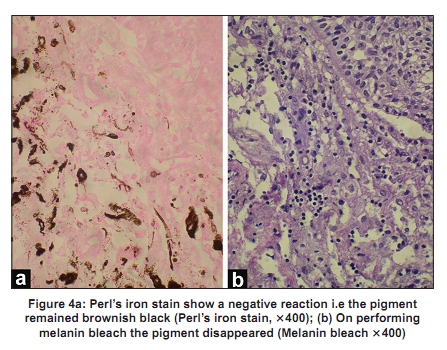
Code Number: ni10047 DOI: 10.4103/0028-3886.60433 Sir, A 33-year-old female presented with a history of amenorrhea for the last seven years, headache of one year and diminution of vision since the last six months. There were no seizures or symptoms of endocrine dysfunction. The diminution of vision was more in the left eye. The magnetic resonance imaging (MRI) showed a sellar, suprasellar lesion with a cystic component measuring 4.7 x 2.8 x 4.2 cms extending up to the anterior part of the third ventricle [Figure - 1]a. A pterional craniotomy and decompression of the tumor was done. The sample was sent to an outside hospital for evaluation and a histopathological diagnosis of an adamantinomatous craniopharyngioma was given without mention of any melanin pigment. The patient presented after eight years with similar complaints. MRI this time revealed a well defined dumbbell shaped sellar, suprasellar mass lesion measuring 3.4 x 3 x 4.9 cms, predominantly cystic with contrast enhancing solid component [Figure - 1]b, extending inferiorly into the sellar, superiorly into the third ventricle causing mild hydrocephalus and posteriorly into the interpeduncular cistern and left temporal lobe. Tumor decompression was done and an Ommaya chamber was placed in the residual cyst. The specimen was sent for histopathological evaluation to the Department of Pathology, Sri Sathya Sai Institute of Higher Medical Sciences. On light microscopy, the tumor was predominantly cystic lined by squamous cells resembling epidermoid cyst with a few foci showing odontogenic epithelium, squamous nests, dystrophic calcification and wet keratin [Figure - 2]. There was subepithelial fibrosis with focal collections of chronic inflammatory cells including foamy macrophages. In addition, granular brown black pigment was seen near the wet keratin, between the inflammatory cells and inside a few squamous cells few tumor cells [Figure - 3]a and b. The pigment was negative on Perl′s iron stain [Figure - 4]a. Following Schmorl′s technique of melanin bleach, the pigment disappeared [Figure - 4]b. On the basis of histomorphological features and special stains a diagnosis of melanotic craniopharyngioma, sellar, suprasellar region was given. Melanotic craniopharyngiomas are extremely rare. Review of literature revealed only three cases [Table - 1]. [1],[2] In the melanotic craniopharyngioma it can be presumed that due to the embryologic similarity between the former and odontogenic tumors; the melanotic cells arose from cells analogous to the paradental epithelium. It is also proposed in literature that these tumors may possibly become pigmented by melanin transfer from leptomeningeal melanocytes or contain entrapped leptomeningeal melanocytes as described for some melanin harboring meningiomas. [3] It should be noted though that many of the neuroepithelial and glial tumors do rarely show presence of melanocytic differentiation. [4] It is very interesting to note that all the reported cases and the present case occurred in dark complexioned people. As suggested by the previous authors, this fact of the race and skin color being one of the contributing factors in the development of this rare variant needs to be evaluated further. However, due to the rarity of this variant it is difficult to establish this fact at this juncture. To conclude, we report an extremely rare case of melanotic craniopharyngioma in a young female, which to the best of our knowledge is the fourth case in the literature. References
Copyright 2010 - Neurology India The following images related to this document are available:Photo images[ni10047t1.jpg] [ni10047f4.jpg] [ni10047f3.jpg] [ni10047f2.jpg] [ni10047f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}