 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 58, No. 1, January-February, 2010, pp. 166-167 Neuroimage Spontaneous rupture of an intracranial teratoma Chen Xuzhu1 , Jiang Tao2 , Wang Junmei 3 , Dai Jianping1 1 Departments of Neuroimaging, 2 Neurosurgery, 3 Neuropathology, Beijing Tiantan Hospital, Capital Medical University, Beijing, China Correspondence Address: Dr. Dai Jianping, Department of Neuroimaging, Beijing Tiantan Hospital, Capital Medical University, Beijing, P. R. China. Date of Acceptance: 23-Oct-2009
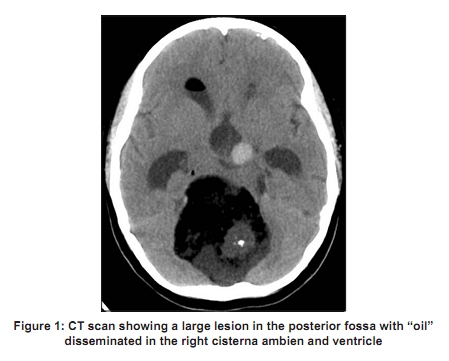
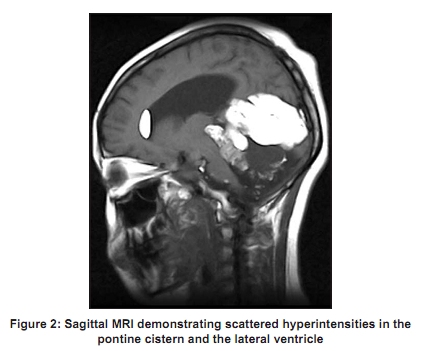
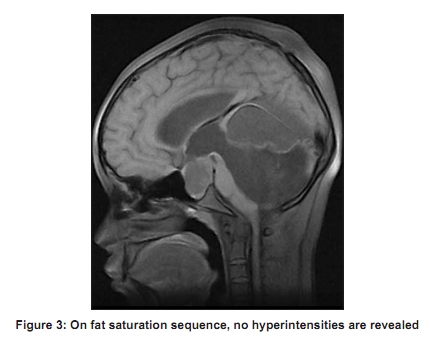
Code Number: ni10049 DOI: 10.4103/0028-3886.60391 Teratoma rupture has been reported in various regions such as the omental sac, [1] mediastinum, [2] pelvic cavity, [3] occipitocervical region, [4] and sacrococcygeal area. [5] To the best of our knowledge, rupture of intracranial teratoma has not been reported to date. We present a case of spontaneous rupture of a large intracranial teratoma. A 16-year-old female patient presented with six months history of headache and dizziness. Her medical history was unremarkable and she did not have any history of trauma. On examination, the left nasolabial groove was superficial and there was a decrease in the angle on the left side of her lips. The uvula deviated to the right side and there was a loss of pharyngeal reflex on the right side. She also had ataxia. Computed tomography (CT) scanning revealed a large lesion in the posterior fossa and the suprasellar region with a maximum diameter of 9.35 cm. This lesion was mostly composed of fat with attenuation value of -36 HU. The solid part of the lesion was heterogeneous in density with multiple calcifications or ossifications within it. Scattered "oil" was seen in the pontine cistern, bilateral cisterna ambiens, and bilateral ventricles, suggesting rupture of the tumor [Figure - 1]. Magnetic resonance imaging (MRI) showed a large lesion in the posterior fossa and the posterior part of the third ventricle. It had linear, dot-like and patchy hyperintensities and irregular hypo intensities. Patchy and dot-like hyperintensities were shown in the bilateral ventricles and cisterns on T1 weighted images (T1WI) [Figure - 2]. On fat saturation sequence, there were no high signals in the tumor, cisterns and ventricles [Figure - 3]. Intraoperatively, the intracranial tumor was hairy in parts and soft in texture with scant blood supply. The inferior part of the tumor was yellow and white in color and composed of oil and fat. The superior part of the tumor was tenacious in texture and yellow in color with septa and calcifications. The tumor was subtotally resected. Histopathological examination confirmed the diagnosis of teratoma. The patient′s recovery was uneventful and she was discharged on the seventh postoperative day. Teratoma, a type of germ cell tumors, makes up 2-4% of intracranial tumors in children. [6] The etiology and pathogenesis of intracranial teratomas are not wholly understood. Some authors insist that these tumors arise from misplaced primordial germ cells, which are embedded in or near the midline structures in the head. Others think the tumors may not originate from one single type of cell such as the primordial germ cells. [7] Pathophysiologically, the mechanism of teratoma rupture remains unclear. In the mediastinum, proteolytic or digestive enzymes derived from the tumor have been proposed as the cause. [8] In the ovary, rupture of mature cystic teratoma may be the result of primary perforation of the tumor. [9] These mechanisms may or may not explain intracranial teratoma rupture. Acknowledgment We thank Miss Ally Chuan Xiang, from King′s College London School of Medicine, 2 nd Floor, Henriette Raphael House, Guy′s Campus, London Bridge, London, SE1 1UL, UK, for her English editing. References
Copyright 2010 - Neurology India The following images related to this document are available:Photo images[ni10049f2.jpg] [ni10049f1.jpg] [ni10049f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}