 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
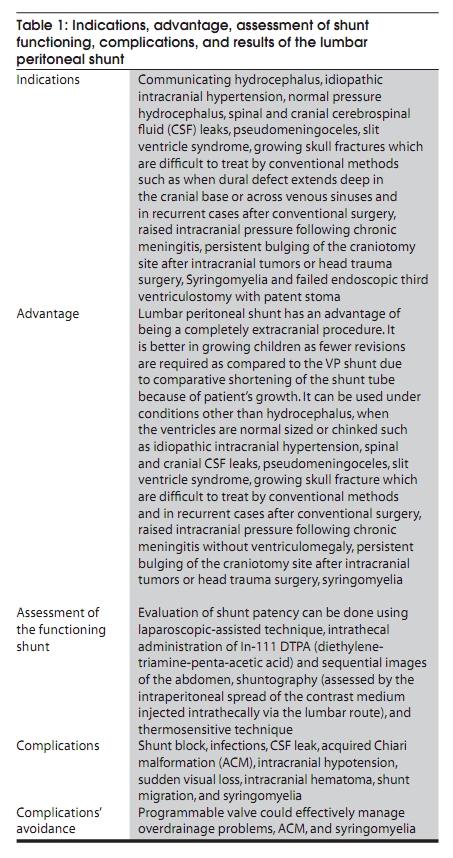
Neurology India, Vol. 58, No. 2, March-April, 2010, pp. 179-184 Review Article Lumbar peritoneal shunt Yad R Yadav, Vijay Parihar, Mallika Sinha Neurosurgery Unit, NSCB Medical College, Jabalpur, Madhya Pradesh, India Correspondence Address: Yad R Yadav, 105, Nehru Nagar, Opposite Medical College, Jabalpur, Madhya Pradesh, India, yadavyr@yahoo.co.in Code Number: ni10052 PMID: 20508332 DOI: 10.4103/0028-3886.63778 Abstract A lumbar peritoneal (LP) shunt is a technique of cerebrospinal fluid (CSF) diversion from the lumbar thecal sac to the peritoneal cavity. It is indicated under a large number of conditions such as communicating hydrocephalus, idiopathic intracranial hypertension, normal pressure hydrocephalus, spinal and cranial CSF leaks, pseudomeningoceles, slit ventricle syndrome, growing skull fractures which are difficult to treat by conventional methods (when dural defect extends deep in the cranial base or across venous sinuses and in recurrent cases after conventional surgery), raised intracranial pressure following chronic meningitis, persistent bulging of craniotomy site after operations for intracranial tumors or head trauma, syringomyelia and failed endoscopic third ventriculostomy with a patent stoma. In spite of the large number of indications of this shunt and being reasonably good, safe, and effective, very few reports about the LP shunt exist in the literature. This procedure did not get its due importance due to some initial negative reports. This review article is based on search on Google and PubMed. This article is aimed to review indications, complications, results, and comparison of the LP shunt with the commonly practiced ventriculoperitoneal (VP) shunt. Shunt blocks, infections, CSF leaks, overdrainage and acquired Chiari malformation (ACM) are some of the complications of the LP shunt. Early diagnosis of overdrainage complications and ACM as well as timely appropriate treatment especially by programmable shunts could decrease morbidity. Majority of recent reports suggest that a LP shunt is a better alternative to the VP shunt in communicating hydrocephalus. It has an advantage over the VP shunt of being completely extracranial and can be used under conditions other than hydrocephalus when the ventricles are normal sized or chinked. More publications are required to establish its usefulness in the treatment of wide variety of indications.Keywords: Cerebrospinal fluid shunt, hydrocephalus, lumbar peritoneal shunt, ventriculoperitoneal shunt Introduction Communicating hydrocephalus secondary to an infective cause is quite common in countries like India while it is more frequent following subarachnoid hemorrhage (SAH) in western countries. Shunt surgery has been found to be effective in such hydrocephalus. A lumbar peritoneal (LP) shunt has an advantage of being an entirely extracranial operation. It is a very effective and safe method of treatment in communicating hydrocephalus compared to the ventriculoperitoneal (VP) shunt. [1],[2],[3] A LP shunt is also effective under some nonhydrocephalus conditions. Initial reports of very high complications have put this procedure into disrepute [4],[5] which has led to underutilization of this procedure. In spite of its use in a wide variety of indications only few reports about LP shunts exist in the literature. We are therefore reviewing the indications, results, and complications of this procedure. Indications A LP shunt is indicated under a large number of conditions as shown in [Table 1]. It is contraindicated in obstructive hydrocephalus. Communicating hydrocephalus A LP shunt has been found to be quite effective and comparatively safe in communicating hydrocephalus. [1],[2] Communicating hydrocephalus is quite common in tubercular meningitis (TBM), other chronic infections, postpyogenic meningitis, and SAH. It is also seen following trauma and surgery. Idiopathic intracranial hypertension Idiopathic intracranial hypertension (IIH) is a condition that usually affects young, obese women. Management is aimed at controlling symptoms of increased intracranial pressure (ICP) and prevention of visual failure due to papilledema. A common surgical treatment for IIH is the insertion of a LP shunt. It is a very effective procedure to treat this condition when conservative treatment fails and the vision is threatened. [1],[6],[7],[8],[9],[10],[11] Normal pressure hydrocephalus Normal pressure hydrocephalus (NPH) is considered to be a treatable form of dementia. A LP shunt has been found to be effective in NPH. [12],[13] Spinal cerebrospinal fluid leaks Cerebrospinal fluid (CSF) leak can occur following spinal surgery or penetrating trauma. Such fistulas are sometimes refractory to direct repair, external drainage, and blood patches. A LP shunt is effective in these difficult situations. [1],[14] Cranial base cerebrospinal fluid leaks A LP shunt could be used in CSF rhinorrhea following either cranial injury, skull base surgery or of unknown etiology. This is one of the techniques to manage such patients when direct closure of fistula fails. This is also indicated in CSF rhinorrhea with raised intracranial pressure. [1],[11],[15] Pseudomeningoceles Pseudomeningoceles can occur after spinal and posterior cranial fossa surgery. A LP shunt is an effective treatment under these conditions. [1],[11],[14] Slit ventricle syndrome Slit ventricle syndrome (SVS) has been described in hydrocephalus patients who continue to have shunt malfunction-like symptoms in the presence of a functioning shunt system and small ventricles on imaging studies. A LP shunt is indicated in a subset of patients with SVS who are symptomatic with high ICP. It is postulated that this subgroup of patients previously treated with VP shunting behave in a fashion similar to pseudotumor cerebri patients and such patients respond well to a LP shunt. [16],[17],[18] Growing skull fracture A LP shunt is indicated in growing skull fractures which are difficult to treat by conventional methods such as when the dural defect extends deep in the cranial base or across venous sinuses and in recurrent cases after conventional surgery. It should be done when bulging disappears after the lumber puncture. [1],[19] Yadav et al. reported a good outcome after a LP shunt under this condition. Its counterpart, a VP shunt, has also been used for the treatment of craniocerebral erosion (growing skull fracture) in difficult cases and recurrent cases after conventional surgery [20],[21] but the VP shunt procedure is difficult when ventricles are not dilated. Raised intracranial pressure following chronic meningitis Elevated ICP in patients with meningitis is a significant source of morbidity and mortality. Use of early LP and VP shunts in the management of elevated ICP can ameliorate the sequelae of elevated ICP. [22],[23] Failed endoscopic third ventriculostomy with a patent stoma Hydrocephalus can be classified as purely obstructive, purely communicating, or due to combinations of pathologies (obstruction in addition to defective absorption). Endoscopic third ventriculostomy (ETV) as an alternative to shunt procedures is an established treatment for obstructive hydrocephalus. However, patients who have combination of pathologies (complex hydrocephalus) could result in the failure of ETV in spite of a patent stoma due to defective CSF absorption or impaired CSF permeation through subarachnoid space. A LP shunt is effective in the treatment of such patients. [24] Persistent bulging of the craniotomy site after intracranial tumors or head trauma operations A LP shunt is quite effective in patients with bulging craniotomy without ventriculomegaly. Such patients could have features of raised ICP. [11] These patients usually do not have dilated ventricles where a VP shunt is very difficult. Syringomyelia Although a valveless LP shunt may expose patient to the risk of symptomatic ACM and syringomyelia, a LP shunt with an adjustable pressure valve could successfully manage such complications. [25] Bret et al.[11] and Vassilouthis et al. [26] performed a LP shunt successfully for the primary treatment of syringomyelia associated with progressive myelopathy. Park et al. suggested that CSF moves under pressure into the spinal cord, contributing to the formation and maintenance of the syrinx. They found that the LP shunting combined with myelotomy could result in the shrinkage of the syrinx. [27] Procedure The introduction of a LP shunting system may be accomplished through a variety of surgical techniques. A surgeon is best advised to use the method which is best suited to his/her own practice and training. A shunt could be in a single-piece system or a two- or three-piece system. Here we are describing the technique of a two-piece system (lumbar and peritoneal end). A 0.5-1 cm skin incision is given between the spinous process of L4-5 or L5-S1. We usually give a 1-2 cm paraspinal incision which prevents incision dehiscence due to pressure especially in malnourished and unconscious patients. A Tuohy needle can be inserted in the midline after the paraspinal incision. The head end of the table is temporarily elevated 30° to increase the pressure in the lumbar subarachnoid space. A fourteen-gauge Tuohy needle is inserted into the lumbar subarachnoid space with the bevel-pointed cephalad. The lumbar end of the catheter is passed through the Tuohy needle. The operating table is tilted back to the normal position. The needle is withdrawn over the catheter. The extra length of the catheter is cut. A single suture collar is placed around the catheter in the lumbar area and sutured to the subcutaneous tissue to hold the catheter in place. A small incision is made in the flank and the subcutaneous catheter passer with the obturator in place is passed through the flank incision. The obturator is removed and the distal end of the peritoneal catheter is inserted into the lumbar opening of the subcutaneous catheter passer. The subcutaneous catheter passer is withdrawn over the catheter leaving the flank portion in place. A small skin incision is made 2 cm below the umbilicus and 3 cm away from the midline. The subcutaneous catheter passer with the obturator in place is inserted from the abdominal incision to the flank incision. The obturator is removed and the peritoneal end is inserted into the flank opening of the catheter passer. The catheter is passed through the passer. The shunt can be inserted into the peritoneal cavity using a peritoneal trocar. An Allis clamp on the aponeurosis is secured and firm outward traction on the abdominal wall is applied. The trocar is inserted through a small stab incision in the superficial layer of the aponeurosis into the peritoneal cavity, while continued outward traction is applied on the Allis clamp. The trocar is removed after insertion. The catheter can also be inserted into the peritoneal cavity under direct vision. A suture collar is placed around the catheter tubing. The collar is sutured to the subcutaneous tissues. All incisions are closed in the usual manner. The thecal end of the shunt is smaller in diameter as compared to the peritoneal end. The Chhabra LP shunt comes with a Tuohy needle. It has a lumbar end which is radiopaque which has an outer diameter of 1.5 mm and an inner diameter of 0.7 mm. The proximal end of the lumbar end bears multiple holes and it is marked at 5, 10, and 15 cm distance from the proximal perforated tip. The lumbar end can pass through the 14-gauge Tuohy needle. The peritoneal end is also radiopaque with a 2.5 mm outer diameter and a 1.3 mm inner diameter. The peritoneal end catheter tip has two pairs of slit valve. Other shunt systems such as Spetzler, Codman, Medtronics, Aesculap, etc. are also available commercially. Programmable/adjustable valves are also commercially available such as Codman Hakim, Medtronics, Aesculap, Phoenix, Integra, etc. Use of a programmable shunt can significantly increase the probability of shunt implantation being a one-time procedure. If the pressure setting of a fixed pressure shunt proves to be a mismatch after surgery, causing underdrainage or overdrainage complications, the patient must undergo a complete or partial shunt revision, sometimes more than once. This is a limitation of all fixed pressure shunts. The opening pressure of programmable shunts can be changed via an external magnet so that surgery is not necessary for a pressure change. The one downside of a programmable shunt is that large magnetic fields can change the pressure setting. As a result, if an MRI is needed the shunt will need to be reprogrammed immediately following the MRI. This does not mean that an MRI cannot be done; it just means that the shunt needs to be reprogrammed. LP shunt placement requires access to the lumbar theca in the lateral position and peritoneal end in the supine position. This position change could be bothersome, especially in heavy patients. Shimizu et al. developed a transportation board to facilitate changing the patient position while keeping the surgical drapes in place. [28] To avoid this change in position, some authors have placed the peritoneal end in the lateral position using a laparoscopy-assisted technique. [29],[30] Goitein et al. described single-trocar laparoscopy-assisted placement of peritoneal shunts. [31] The direct placement of a peritoneal catheter from back by the laparoscopy-assisted technique was described by Johna et al. [3] Kubo et al. developed a method for the retroperitoneal placement of a LP shunt with the aid of endoscopic monitoring. [32] Assessment of the Functioning Shunt The placement of the LP shunt tube and the evaluation of its patency can be done using a laparoscopy-assisted technique. [33,34] The intrathecal administration of In-111 DTPA (diethylene-triamine-penta-acetic acid) and sequential images of the abdomen and of the head can be used to assess shunt patency. [12] LP shunt patency can be assessed by LP shuntography in which patency of the shunt can be judged by the intraperitoneal spread of the contrast medium injected intrathecally via the lumbar route. [35],[36] A thermosensitive determination technique is another method in which patency of the shunt can be assessed by definite temperature changes. [37] Postoperative Imaging after LP Shunting A decrease in the size of the ventricles occurs very slowly in about few weeks to months after a successful shunt. Patients with chronic dilatation of ventricles take longer time and in some cases the ventricles do not become normal. The clinical status along with the comparison of pre- and postoperative imaging is more important than the ventricle size alone in a single imaging. Failure to decrease in size of ventricles or increase in size with clinical deterioration or failure to improve is suggestive of shunt malfunction. Comparison of LP Shunt Results with a VP Shunt A LP has an advantage of being a completely extracranial procedure. It is better in growing children as fewer revisions are required as compared to the VP shunt due to comparative shortening of the shunt tube because of patient′s growth. Aoki reviewed 207 cases of LP shunt and 120 comparable cases of VP shunt and found that the incidence of infection and malfunction with a LP shunt is significantly lower than that with a VP shunt. They also observed that the LP shunt is also indicated for pediatric patients, although a relatively higher incidence of malfunction was noted compared to the adults. [2] They reported a very low incidence of ACM after the LP shunt. Wang et al. reported that the placement of LP shunts with a horizontal-vertical valve for the treatment of communicating hydrocephalus seems to be a safe procedure. Serious overdrainage complications such as subdural hematoma (SDH) were not observed with the valve system. The horizontal-vertical valve was associated with minor complications but it was effective in reducing the incidence of overdrainage complications. [38] Rekate also found that LP shunts may be used for specific indications without excessive risk of hindbrain herniation. [39] Yadav et al. found a low incidence of shunt block in the LP shunt as compared to the VP shunt; they also observed a very low incidence of ACM (0.5%). On the other hand, Kim et al. observed that a VP shunt is the better choice compared to LP shunts in treating chronic hydrocephalus after aneurismal SAH. [40] Complications Shunt block, infections, and CSF leak are quite common in LP shunts. [1],[2] Sudden visual loss can occur due to an acute rise in ICP because of shunt block. [41] The incidence of ACM was very high in Chumas et al.[4] and Payner et al. [5] series while it was very low (0.5%) in Yadav et al.[1] and Aoki et al. (1%) series. [2] Rekate et al. [39] did not come across any risk of ACM in children; they used the valve system in majority (84%) of patients. Lam et al. also found secondary ACM rarely after the LP shunt. [42] Riffaud et al. observed that the valveless LP shunt may expose the patient to the risk of symptomatic ACM and syringomyelia. They suggested a LP shunt with an adjustable valve to prevent such complications. [25] It is evident from these reports that the overdrainage complications such as ACM can be avoided by a programmable shunt. Liao et al. described intracranial hypotension from the leakage of CSF through a defect in the lumbar dura created by the shunt catheter in a LP shunt. [43] Tension pneumocephalus may develop following continuous lumbar drainage [44] but such complication has not been described in a LP shunt procedure. Acute SDH is a rare complication of LP shunts. [45] These complications can be prevented by an adjustable valve. Shunt migration after LP shunt procedures can occur upward into the spinal subarachnoid space and downward into the abdominal cavity. Cranial migrations are less common than downward migration into the abdominal cavity. Defects of the fixation devices in the shunt system are considered the main cause. Raised abdominal pressure and a strong force produced by lumbar movements are supposed to be related to upward migration. [46],[47] A rare complication of cranial migration of the catheter in the posterior fossa has been reported. [48] There were reports of back pain with or without sciatica, hamstring tightness, foot deformities, lumbar hyperlordosis, lordoscoliosis, and scoliosis in old shunt systems. These deformities are postulated to be the result of arachnoiditis involving the conus medullaris and lower lumbar roots. [49] Subarachnoid hemorrhage and intracereebral hematoma have been reported following a LP shunt. [50] Shunt infection varies from 1% to 9% in various series. [1],[2],[18],[38],[51] The incidence of shunt revision ranges from 11% to 50% in various series. [1],[2],[38] Overdrainage complications were recorded in 1-15% patients. [2],[38],[51] It was seen in 15% patients in the LP shunt group without a valve while the LP shunt with a valve did not develop any overdrainage complications. [38] Overdrainage complications can be avoided by a programmable valve. [25],[38],[39],[52] Shunt blocks were seen in 4-14% cases. [1],[2],[51] References
Copyright 2010 - Neurology India The following images related to this document are available:Photo images[ni10052t1.jpg] |
| |||||||||


{kind=link}