 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
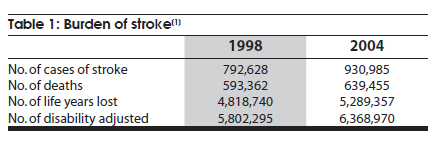
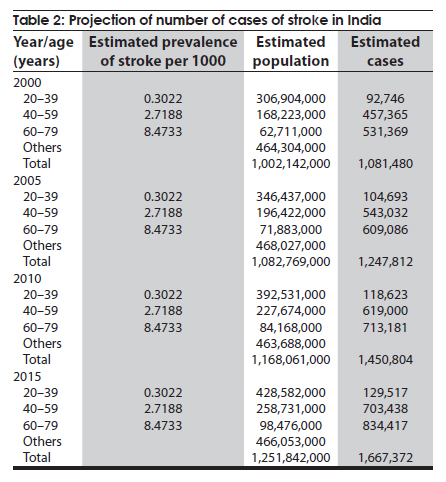
Neurology India, Vol. 58, No. 3, May-June, 2010, pp. 343-350 Indian Perspective Stroke in young: An Indian perspective Kameshwar Prasad, Kapil K Singhal Department of Neurology, All India Institute of Medical Sciences, New Delhi, India Date of Acceptance: 15-Apr-2010 Code Number: ni10096 PMID: 20644260 Abstract The issue of stroke in young in India has long been of interest to neurologists in the country. The age group for stroke in young has been variable between different studies but perhaps should be restricted to 15-49 years as this age group tends to have a unique set of causes and risk factors. There is no evidence indicating higher incidence of stroke in young in India than in other countries. Age-specific incidence rates from recent population-based studies from India are comparable to the western populations. Though the traditional risk factors of stroke play a significant role in young age group also, the presence of high number of cryptogenic strokes, cardioembolic and venous strokes makes diagnostic evaluation in this age group more challenging. This review aims at defining the age group for stroke in young, focuses on incidence of stroke in young on the basis of different population-based studies and details the risk factors and diagnostic approach of different stroke subtypes in young.Keywords: Incidence, India, stroke in young Introduction Stroke is a major public health problem. According to World Health Organization (WHO), stroke has caused about 5.54 million deaths worldwide in 1999 with two-thirds of these deaths occurring in less developed countries. Stroke is also the most common neurological condition causing long-term disability and has enormous emotional and socioeconomic consequences in patients, their families and health services. The latest available estimates from Indian Council of Medical Research (ICMR) indicate that in 2004 there were 930,985 cases of stroke in India with 639,455 deaths and 6.4 million disability adjusted life years (DALY) lost [1] [Table - 1]. In India the incidence of stroke is likely to rise in the coming years due to:
Age and Stroke Incidence Age has the strongest association with the incidence of stroke. For example, an 80 year old has about 30 times the risk of ischemic stroke than a 50 year old. [3] The age-specific incidence of stroke increases progressively with increasing age. In a systematic review of 15 population-based stroke incidence studies, [4] the rate of total stroke for those aged less than 45 years ranged from 0.1-0.3 per 1000 person years, while for those aged 75-84 years, the range was 12-20 per 1000 person years in most studies. However, the impact of stroke on the individual family and society is strongest when it affects a young individual. Therefore, stroke in young attracts a large share of attention, perhaps disproportionately large. Therefore, in India as well as in other countries, there has been a large body of literature addressing the issues related to stroke in young. This review is an attempt to summarize some of this literature with special reference to the Indian context. Issues Related to Stroke in Young Clinical management as well as epidemiologic perspective raises several issues in relation to stroke in young. Important issues amongst these include the following:
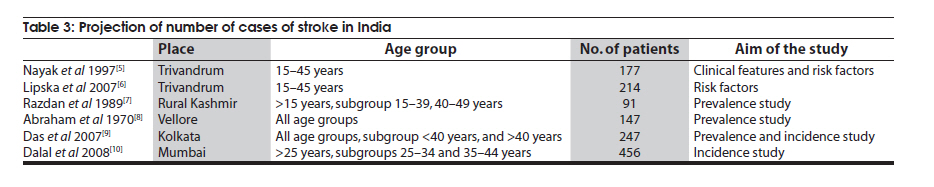
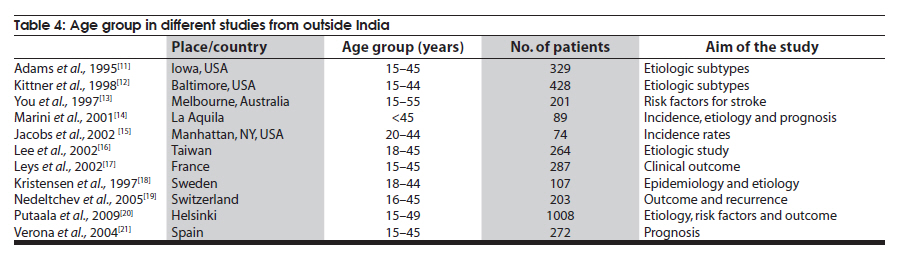
We address these issues in the following paragraphs. Defining 'Young' The age group included in studies on stroke varies widely in the reports published in literature [Table - 3] and [Table - 4]. The lower limit of the age varies from 0 to 25 years in various reports with majority keeping it at 15 years. The upper age limit also varies from 40 to 55 years, majority being around 45 years. The wide variation compromises comparisons across the studies and confounds communication among experts. The rationale for the choice of age group is not given in the reports. In our opinion, the following points need consideration while defining the age category for young.
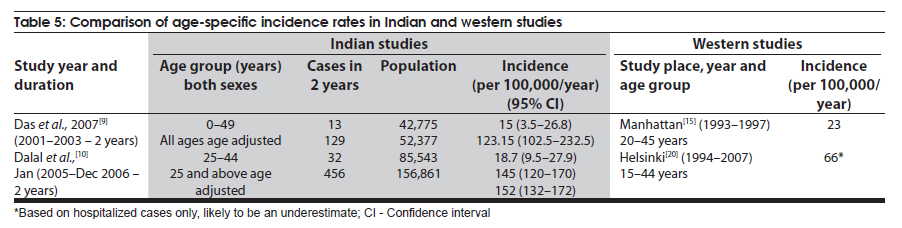
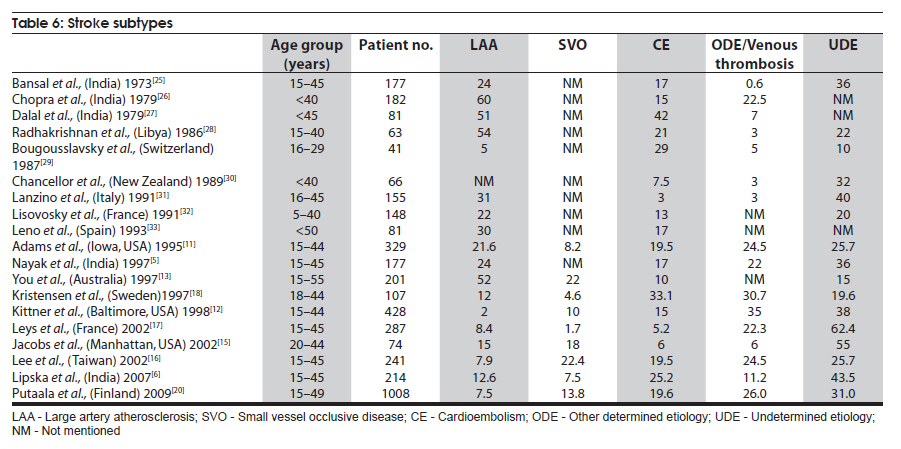
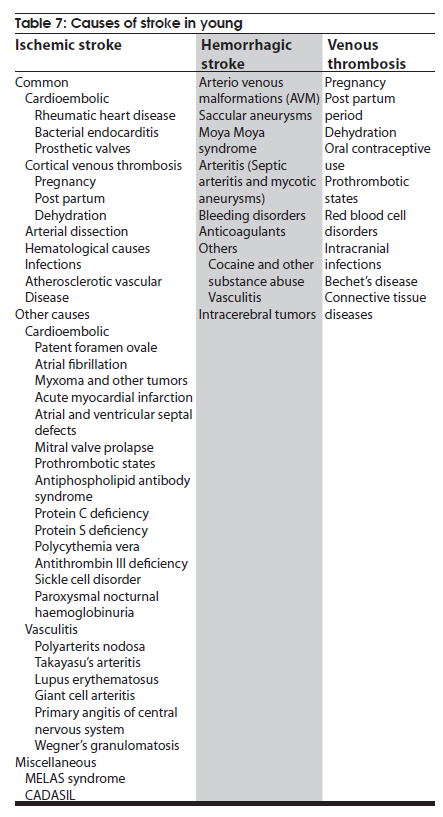
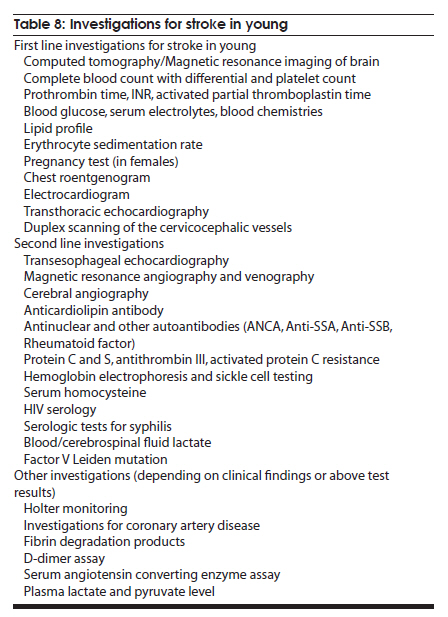
High Susceptibility of 'Young' Indians to Stroke: A Myth Several hospital-based studies on stroke in young adults from India had hypothesized that young Indians are more susceptible to stroke than their counterparts from industrialized countries. In an editorial on the topic in 1997, [22] Prasad had commented 'Indians as a whole are probably more susceptible to stroke than people in industrialized countries and that the magnitude of increased susceptibility is probably similar for the young and older adults … to answer this question, a well designed study is required in India which can be compared to a similar contemporary study in the west'. There are two recent studies [9],[10] from Kolkata and Mumbai that allow us to compare the age-specific incidence between India and other countries. It is clear that young adults in India are not more susceptible to stroke than their counterparts in the west, though Das et al.[9] have noted that for all age groups together standardized rate of stroke incidence (123.5/100,000/year) is higher than that observed in USA (107/100,000/year), European countries (61-111/100,000/year), and Australia (99/100,000/year). These data, together with the studies on Indian immigrants to UK and the USA, suggest that Indians in general may probably be more susceptible to stroke but there is no age-specific higher susceptibility for the young. Previous hospital-based studies from India showing a high proportion of young strokes, ranging between 15 and 30%, were over estimates probably because of a preferential admission policy. One area that remains to be well documented is the incidence of peripartum stroke. There is a strong impression among clinicians that the incidence is several times higher than that in other countries, particularly in industrialized countries. [Table - 5] shows incidence rate in recent Indian and western studies Stroke Subtypes, Risk Factors and Etiology The 'mix' of causes, the proportion with 'no cause' and the outcome of stroke in young varies from one series to the other. While some of the variations may be real, the majority is probably explained by the referral bias, differences in admission policy, in the pattern/availability of emergency services, investigation intensity and diagnostic criteria. All these may change with time as more causes are discovered and new diagnostic technologies become available. No two series are, therefore, strictly comparable. The following paragraphs may be read with this caveat in mind. The prevalence of various risk factors in stroke in young has been analyzed in two studies from India. [5],[6] In a case control study of young stroke patients (age group 15-45 years) with age- and sex-matched hospital and community controls, [6] prevalence of various risk factors was studied. Two hundred fourteen South Indian patients with first acute ischemic stroke and 99 hospital and 96 community controls were included. There was higher prevalence of smoking (odds ratio [OR] 7.77), systolic blood pressure (OR 1.88) and fasting blood glucose (OR 4.55) in patients. High density lipoprotein (HDL) was low and total cholesterol/HDL ratio was high in cases when compared with both hospital and community controls. A unit increase in the ratio of total cholesterol to HDL was associated with doubling of stroke risk. More than three components of metabolic syndrome were present in 12.6% cases when compared to 6% of community controls. Presence of ≥3 components of metabolic syndrome was also strongly associated with stroke (OR 4.76). In another study in 1997, [5] 177 patients with first ever ischemic stroke (age group 15-45 years) were included retrospectively based on hospital data, with 76% male and 24% female patients. Hypertension was present in 18% of the patients, whereas diabetes mellitus was present in 7% only. Sixty nine percent of male patients were smokers. Dyslipidemia in the form of elevated cholesterol was present in 17% and increase in triglycerides was observed in 42% patients. Sridharan et al.[23] analyzed the risk factors in ischemic stroke including the patients of all age groups. Hypertension, ECG abnormality, heart disease of any type, diabetes, smoking and alcohol were associated with stroke. Low HDL and low density lipoprotein (LDL) to HDL ratio was observed among stroke patients. South Asians living in UK are known to have an atherogenic lipid profile, which includes raised triglycerides, low HDL cholesterol and raised lipoprotein a levels. [24] In a study of stroke in the young from Southeast Asia, [16] the most common risk factors observed were hyperlipidemia (53.1%), smoking (49.8%), hypertension (45.8%) and a family history of stroke (29.3%). The presence of hyperlipidemia and hypertension was more commonly seen in patients with small vessel occlusion, large artery atherosclerosis and stroke due to unknown etiology, whereas hyperlipidemia was less commonly associated with cardioembolic stroke. Analysis of prevalence of risk factors in studies of stroke in young from the west reveals prevalence of hypertension from 20 to 60%. [18],[19],[20] In Baltimore Washington Cooperative Young Stroke Study [12] examining 296 incident stroke cases in Black and White adults, hypertension was present in 61% of Black patients. Smoking was observed in 42.6% of White and 56.7% of Black men and 37.0% of White and 47.5% of Black women. In Helsinki Young Stroke Registry [20] which included 1008 first ever patients of ischemic stroke in the age group of 15-49 years, hypertension, smoking and dyslipidemia with high total cholesterol emerged as important risk factors. The prevalence of hypertension increased with increasing age and was seen in 28.3% of patients in 15-44 year age group, whereas it was prevalent in 51.7% of patients in 45-49 year age group. Similarly, 38.4% of patients in 15-44 year age group and 54.5% in 45-49 year age group had increased level of cholesterol. Low HDL was present in 15.3 and 23.9% of the patients, respectively. Increased LDL was also present in 38.4% patients in 15-44 year age group and in 54.5% patients in 45-49 year age group. Smoking as a risk factor was observed in around 47% patients in both the age groups. It appears that the risk factor profile becomes similar to older population with increasing age, the change becoming more apparent at around 44 years of age. In a study of 203 patients of stroke in age group of 15-45 years from Switzerland, [19] hypercholesterolemia (39%) and smoking (46%) were important risk factors. However, hypertension was present in 19% patients only. Increased C reactive protein level was observed in 36% patients. It appears that the risk factors for stroke in Indian population are not different from the western or Southeast Asian population. The traditional risk factors like hypertension, smoking and diabetes are associated with stroke in both young and elderly. The role of dyslipoproteinemia in the pathogenesis of cerebrovascular disease is less certain than that of coronary artery disease; however, increased total cholesterol and increased triglyceride levels have been observed in patients from India and Southeast Asia. Increased level of total cholesterol has been associated with ischemic stroke in young in most of the populations and it does not significantly differ from the Indian subcontinent. In a study on stroke in young from Sri Chitra Tirunal Institute of Medical Sciences and Technology (SCIMST), Trivandrum, [6] patients of ischemic stroke were classified based on Trial of ORG 10172 in Acute Stroke Treatment (TOAST) criteria; 25.2% patients had cardioembolic stroke, 12.6% had large artery atherosclerosis and 7.5% had lacunar infarcts. Strokes due to other determined etiology were 11.2% (7.0% arterial dissection, and one patient each with lupus erythematosus, primary antiphospholipid antibody syndrome and protein S deficiency). Four patients had stroke due to other causes (one case each of Moya moya disease, Takayasu's arteritis, fibromuscular dysplasia and nephritic syndrome). Data from several studies indicate that 21-48% of strokes in the young are caused by atherosclerotic large artery occlusive disease, 10-33% are due to nonatherosclerotic large artery occlusive disease (dissections have comprised 10-20% in some studies), 13-35% are caused by cardioembolism, 3-18% by penetrating artery disease, 8-15% by prothrombotic states and 4-15% by miscellaneous causes. Cryptogenic stroke comprises 7-40% of the cases. In a study by Lee et al., [16] vascular risk factors like hypertension, diabetes, hyperlipidemia were seen more commonly in patients with large artery atherosclerotic disease or small vessel occlusive disease. Cervical artery dissection was one of the relatively common causes of stroke in young. Various studies report that around 6-15% of the patients had carotid artery dissection. Carotid and vertebral artery dissection were seen with a variable frequency. In one study, 24 patients had arterial dissection of 170 [16] patients who underwent angiographic studies, with carotid dissection in 13 and vertebral dissection in 11. The commonest site for carotid dissection was just above the carotid bifurcation. Putaala et al., [20] in a study of stroke in young from Helsinki, reported that 59% of patients with stroke of other determined etiology had cervical or intracranial artery dissection. Out of 155 patients with dissection, 80 had vertebral artery dissection and 67 had internal carotid artery dissection. Other causes of stroke like antiphospholipid antibody syndrome, factor V Leiden mutation, proteins C and S deficiency, antinuclear antibody positivity, systemic lupus erythematosus, fibromuscular dysplasia, migraine-related stroke and other vasculitis were observed in 1-2% of patients. The different subtypes of ischemic stroke in different studies are outlined in [Table - 6]. The common causes of cardioembolic stroke include rheumatic heart disease, paradoxical embolism due to patent foramen ovale (15-37% of cardioembolic strokes), atrial fibrillation (10-14% of cardioembolic strokes), mitral valve prolapse (1-38%), mechanical prosthetic valves, dilated cardiomyopathy, atrial myxoma, congestive heart failure and sick sinus syndrome. Various causes that need consideration in a young patient with stroke are outlined in [Table - 7]. Genetics Several candidate genes have been found to be associated with stroke. Angiotensin converting enzyme (ACE) insertion/deletion polymorphisms, methylenetetrahydrofolate reductase (MTHFR) mutations, apolipoprotein E polymorphisms and phosphodiesterase 4D (PDE4D) gene variants have been studied in Indian population. In a case control study, apolipoprotein E genotypes were studied in patients of stroke. [34] A high frequency of apo ε 4 allele (30% in cases and 11% in controls) was observed (OR 4.2 ). The authors concluded that presence of apo ε 4 allele along with elevated triglycerides, hypertension and age could predict the development of stroke. In another case control study from Hyderabad, [35] angiotensin converting enzyme deletions/insertions were studied. The ORs for ID genotype, DD genotype and D allele as an independent risk factor for ischemic stroke were 2.89, 3.68 and 2.13, respectively. Presence of D allele was also associated with intracranial atherosclerosis. MTHFR C677T mutations were studied in patients with both arterial and venous stroke with elevated homocysteine levels. [36] The prevalence of the mutated homozygous and heterozygous C677T MTHFR genotype in the patients with arterial stroke was 1.4 and 31.88%, respectively. Their frequency was 16.6 and 33.3% in venous stroke. The genotyping results from controls showed that there was only one heterozygote out of the 49 studied. The mutated allele was present in 25.4% of patients in age group of 15-50 years. OR for the probability of the C677T MTHFR gene mutation in the patients versus control group was 22.29 indicating that C677T MTHFR mutation is strongly associated with arterial stroke especially in young adults. PDE4D gene seems to contribute to the risk of stroke in carriers independent of other genetically based risk factors. [37] The association of PDE4D with stroke was investigated in a South Indian population. [38] PDE4D gene polymorphisms were studied in 250 cases and controls. Single nucleotide polymorphism (SNP) 83 showed significant association with stroke in the population under study, whereas SNPs 87 and 32 were monomorphic. SNP 83 was found to be significantly associated with two stroke subtypes, intracranial large artery atherosclerosis (the most frequent subtype in the population) and small artery occlusion. The role of G20210A in ischemic stroke patients was studied in a case control study from South India. [39] None of the study subjects were either heterozygous or homozygous for this gene mutation as indicated by polymerase chain reaction (PCR) analysis. ACE gene polymorphism is presently being studied in patients of both ischemic and hemorrhagic stroke with age-matched controls. The above studies point toward an association between ACE gene mutations, MHTFR mutations and PDE4D polymorphisms with increased risk of stroke. Investigations The investigational approach to stroke in young is similar to that for older adults. However, on the basis of differential consideration of causes presented in this review, additional studies are necessary with an emphasis on cardiac disorders, hematologic disorders such as hypercoagulable states, infectious and inflammatory causes, and metabolic or hereditary disorders. A systematic approach is presented in [Table - 8]. Treatment Treatment of stroke in young depends on its cause. The general principle of treatment remains the same as in older adults outlined in the National Guidelines for Management of Stroke in India. [40] However, some points deserve particular attention: Venous stroke Antithrombotic treatment is aimed at recanalyzing the occluded sinus or vein and preventing propagation of thrombus in patients with venous stroke secondary to cortical venous sinus thrombosis (CVT). Patients with stroke due to CVT (with or without hemorrhagic infarct or secondary cerebral hemorrhage) should be given full dose anticoagulation, initially heparin and then warfarin (INR 2-3), unless there are contraindications. [40] There is no strong evidence to support the use of either systemic or local thrombolysis in CVT. [41] Continuation of anticoagulation for a period of 6-12 months is recommended in survivors of CVT. More prolonged oral anticoagulation is reserved for patients with inherited or acquired prothrombotic disorders. Antiepileptics can be started on patients who had a seizure or a hemorrhagic parenchymal lesion. Intracerebral hemorrhage Treatment for intracerebral hemorrhage in young is similar to that in older adults. Ruptured intracranial aneurysms and AVMs in young adults are usually treated surgically, preferably with excision but possibly radiosurgery, embolization or a combination of both should be considered. For unruptured AVMs, radiosurgery becomes more of a consideration especially for a small AVM that is surgically inaccessible. Consideration is also given for long life expectancy in young patients with AVMs. Rheumatic heart disease Patients with cardioembolic stroke and with atrial fibrillation should be treated with aspirin 300 mg for the first 2 weeks before starting anticoagulation if the stroke is disabling. Patients with prosthetic valves have a significant risk of hemorrhagic transformation, in these patients anticoagulation should be stopped for 1 week and aspirin 150-300 mg should be substituted. [40] Arterial dissection Anticoagulants or antiplatelet agents should be started in patients with stroke secondary to arterial dissection. Endovascular treatment including stent placement over the diseased artery or over the neck of pseudoaneurysm with occlusion of the aneurysm using a coil can be considered in selected patients. [42] Prognosis The prognosis for stroke in young is better than that for older adults with a comparable lesion. The overall average mortality of pregnant patients with cerebral venous thrombosis is approximately 25%. For patients who survive, the prognosis is usually excellent with less risk of persistent neurological deficit than that of the patients with cerebral infarction from arterial lesions. References
Copyright 2010 - Neurology India The following images related to this document are available:Photo images[ni10096t8.jpg] [ni10096t4.jpg] [ni10096t1.jpg] [ni10096t6.jpg] [ni10096t5.jpg] [ni10096t2.jpg] [ni10096t3.jpg] [ni10096t7.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}