 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 58, No. 3, May-June, 2010, pp. 361-370 Review Article Structural and functional neuroimaging in intractable epilepsy Swati Chinchure, Chandrasekharan Kesavadas, Bejoy Thomas Department of Imaging Sciences and Interventional Radiology, Sree Chitra Tirunal Institute for Medical Sciences and Technology, Trivandrum - 695011, India Date of Acceptance: 17-Jun-2010 Code Number: ni10098 PMID: 20644262 Abstract Medical management remains unsatisfactory in about a third of patients with epilepsy and some of them are candidates for resective epilepsy surgery. Structural and functional neuroimaging plays an important role in the identification of the precise cortical region responsible for seizures and is very crucial for a good surgical outcome. Furthermore, identification of eloquent cortical areas near the region to be resected is essential to avoid postoperative neurologic deficit. The magnetic resonance imaging (MRI) protocol for epilepsy can be individually tailored depending on the seizure semiology and possibly electroencephalography. New MRI techniques demonstrate the structure of the brain in fine detail, help in understanding the underlying pathology, and demonstrate functional activity of the brain with high spatial and temporal resolution. Metabolic imaging techniques, such as positron emission tomography (PET) and single photon emission tomography (SPECT) visualize metabolic alterations of the brain in the ictal and interictal states. In MR-negative epilepsy patients, these techniques may have localizing value. The proper use and interpretation of the findings provided by these new technologies is crucial. In this review article, we discuss various conventional and advanced MRI techniques, interpretation of various findings, and the role of functional imaging modalities, such as functional MRI, PET, and SPECT in the localization of epileptogenic substrate as well as for understanding the pathophysiology, propagation, and neurochemical correlates of epilepsy.Keywords: Epilepsy surgery, functional magnetic resonance imaging, intractable epilepsy, magnetic resonance imaging, positron emission tomography, single photon emission tomography (SPECT) Introduction The international classification of epilepsies and epilepsy syndromes [1] recognizes the dichotomy between age-related idiopathic epilepsies on one hand and symptomatic and cryptogenic (presumed symptomatic) epilepsies on the other. Symptomatic indicates that the epilepsy has a known or suspected etiology. Imaging plays an important role in identifying the pathologic substrate responsible for the seizures in patients with symptomatic epilepsies. Magnetic resonance imaging (MRI) should be the neuroimaging modality in chronic epilepsy, especially in intractable epilepsy, because computed tomography (CT) has a limited role. In a significant number of patients, optimal conventional MRI protocol fails to localize epileptogenic focus resulting in the need for invasive monitoring techniques. In the literature, there is no consensus regarding the optimal MRI protocol for epilepsy workup. In this review, we discuss the optimal MRI protocols as well as newer MRI techniques useful for identifying the epileptogenic focus. We also discuss the usefulness of functional MRI (fMRI) and other functional imaging modalities, such as positron emission tomography (PET) and single photon emission computed tomography (SPECT) in the presurgical workup. Computed tomography MRI has been consistently superior to CT in terms of sensitivity and specificity for identifying the etiology of epilepsy. [2],[3],[4] CT retains a supplementary role to MRI, especially in the recognition of intracranial calcification, which may not be easily identified by MRI. [5],[6] CT is also useful when MRI is unavailable or contraindicated and also is preferable for acutely ill patients because patient accessibility and acquisition time are limiting factors for MR scanning. Magnetic resonance imaging As compared with CT, MRI with its higher sensitivity, better spatial resolution, excellent soft tissue contrast, multiplanar imaging capability, and lack of ionizing radiation and functional information, emerges as the primary modality of choice in the evaluation of patients with epilepsy. The main purpose of neuroimaging in epilepsy is
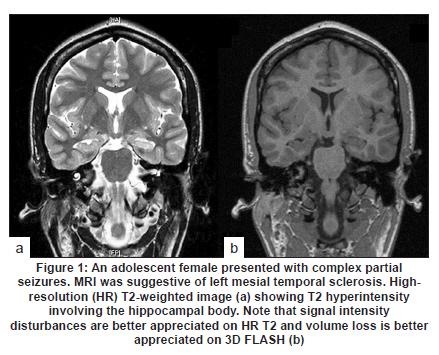
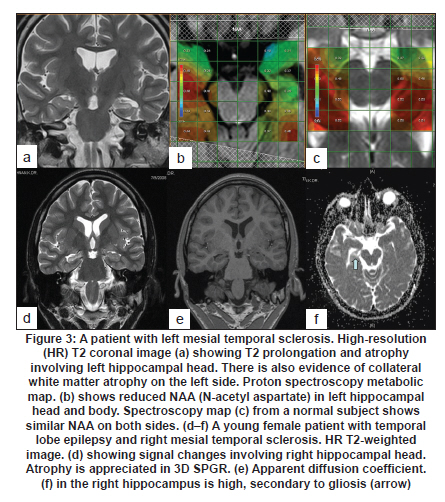
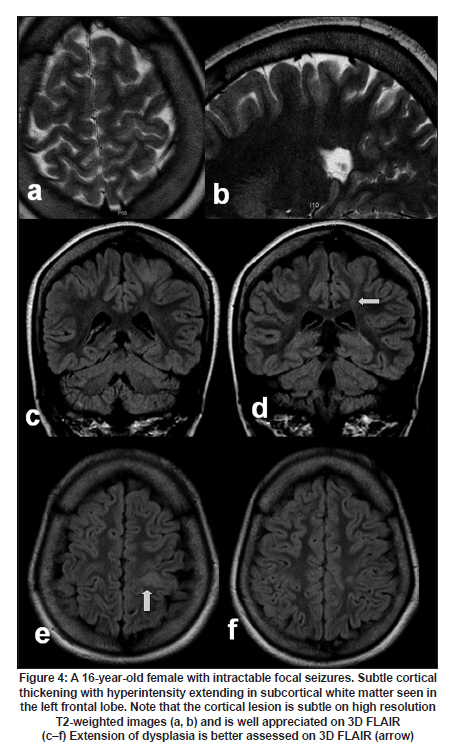
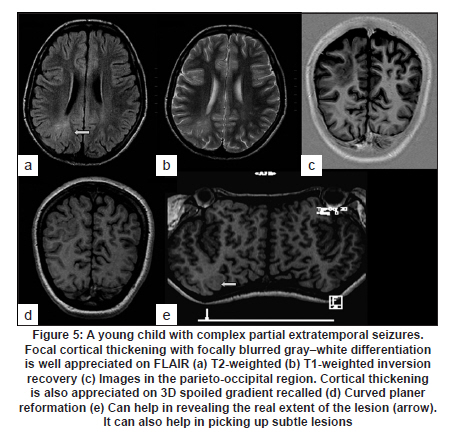
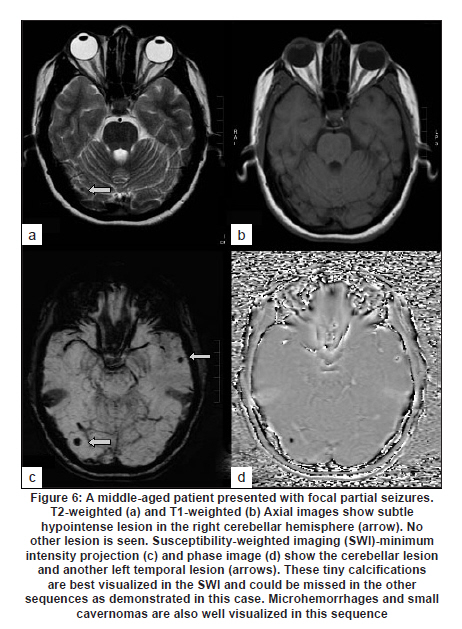
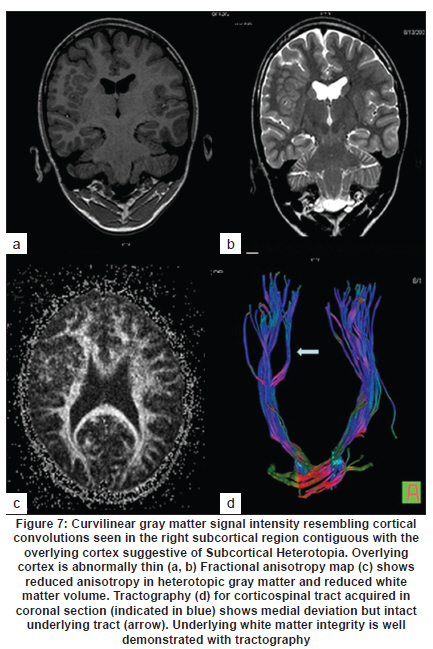
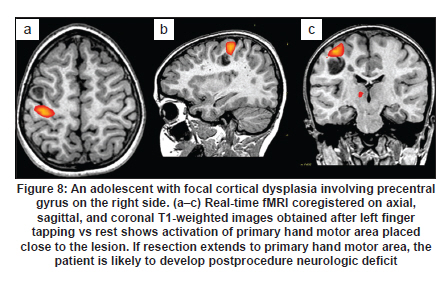
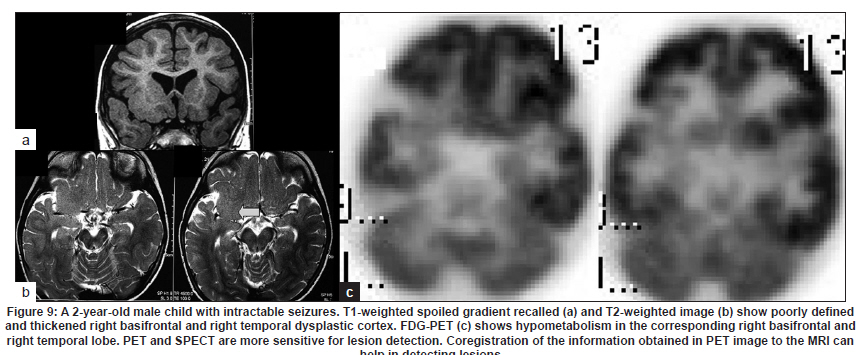
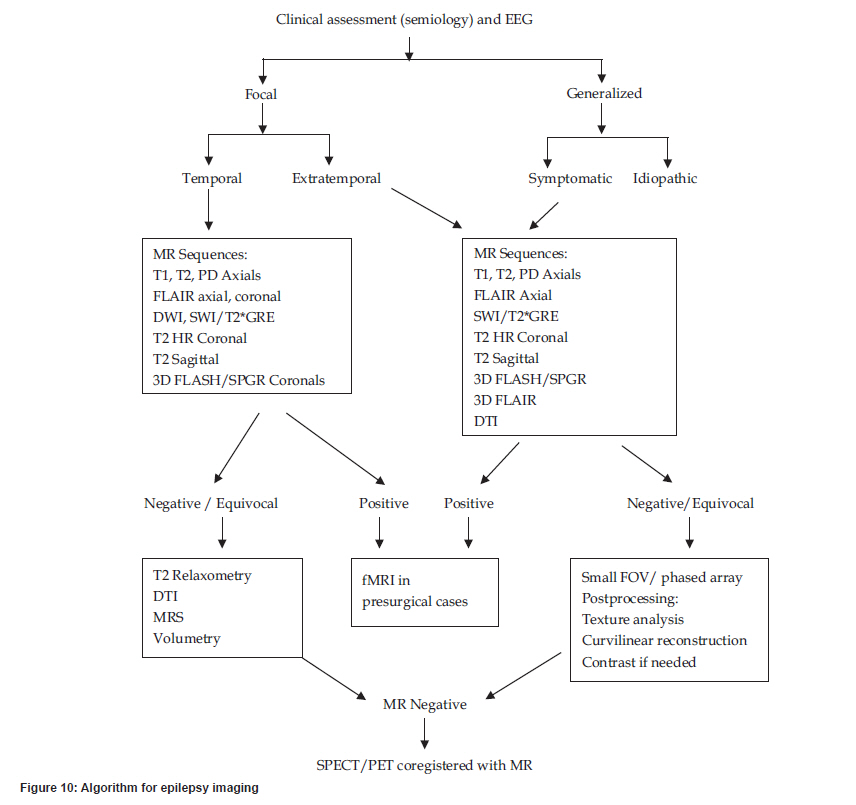
Postoperative seizure control is dependent on MRI identification of a substrate and the nature of the substrate. Postoperative seizure freedom in patients with focal brain lesions is 80%, 62% in patients with hippocampal sclerosis (HS), and 36% in patients with normal MRI. [7] Correlation and concordance of MRI-identified substrate with clinical and electrophysiologic data is essential to avoid a false-positive localization of an epileptogenic substrate. [8] Concordance between noninvasive electrophysiologic data and MRI findings may obviate the need for invasive monitoring. [9] The epileptogenic lesions are mainly of 5 categories: HS, disorders of neuronal migration and cortical disorganization, vascular malformations, tumors, and posttraumatic neocortical gliosis. MRI is the most sensitive and specific means for noninvasive identification of each of these lesions. [6],[10] MRI findings may also indicate whether the patient is a surgical candidate, the type of surgery, and postoperative seizure control. [11] MRI protocol The optimal MRI protocol for the evaluation of patients with epilepsy should depend on clinical characteristics and electrophysiologic findings; temporal vs extratemporal epilepsy. Conventional sequences should include the following: axial T1-weighted spin echo, axial T2-weighted fast spin echo, axial proton density, axial 2D T2 FLAIR, T2FNx01GRE/susceptibility-weighted imaging (SWI), sagittal T2 fast spin echo, high-resolution (HR) T2 coronals, and at least one 3D sequence (3D spoiled GRE/FLASH). When the seizure semiology and electroencephalography (EEG) findings are suggestive of mesial temporal lobe epilepsy, the additional sequences may include T2 relaxometry and hippocampal volumetry. In patients with clinical extratemporal substrate, the protocol may include 3D T2 FLAIR sequence. A postcontrast 3D T1-weighted fat-suppressed sequence may be included in patients with late onset epilepsy. The newer advanced techniques that can be used to further delineate the epileptogenic substrate are magnetization transfer imaging (MTI), magnetic resonance spectroscopy (MRS), diffusion-weighted imaging (DWI), diffusion tensor imaging (DTI), SWI, and T2 mapping. For functional neuroimaging, the available modalities include fMRI, PET, and SPECT. fMRI is used for eloquent cortex mapping and language lateralization, whereas PET and SPECT can demonstrate subtle functional changes related to epilepsy that may ultimately enable the detection of epileptogenic areas not demonstrable on MRI. Structural neuroimaging in temporal lobe epilepsy HS or mesial temporal sclerosis (MTS) refers to an entity of neuronal loss and atrophy with associated gliosis involving the hippocampus. It is a progressive disorder with evidence of premature accumulation of corpora amylacea in the hippocampus in medically refractory temporal lobe epilepsy with HS. [12] HS is the most common pathologic abnormality associated with medically intractable temporal lobe epilepsy. Volume loss and signal changes in the hippocampus are the 2 principle and consistent MRI features of HS. Because of anatomic orientation of hippocampus, MRI findings are best identified on coronal scans perpendicular to the long axis of hippocampus. Thin slices improve confidence in detecting asymmetry. The best conventional MR sequences to show alterations in the normal cytoarchitecture within hippocampus are inversion recovery and HR fast spin echo images. [13] Real-valued ("true") inversion recovery, the image is reconstructed in real rather than magnitude mode, provides exceptionally good gray-white contrast and is a good sequence for internal cytoarchitecture. [14] Hippocampal hyperintensity is best visualized in HR fast spin echo images with T2-weighted scans [Figure - 1]a. Increased signal is thought to reflect gliosis. Fast spin echo MR enables accurate definition of the extent of hippocampal sclerosis in patients with temporal lobe epilepsy. [15] The signal changes in the hippocampus are highly sensitive for HS and occur in 84-100% patients with HS. [16],[17] The 3D spoiled GRE/FLASH sequence provides good information regarding hippocampal volume loss on the side of sclerosis [Figure - 1]b. The detection of multiple primary imaging criteria (loss of hippocampal volume, internal architecture, and signal change) and secondary imaging criteria (atrophy of ipsilateral mammillary body and fornix, atrophy of collateral white matter, atrophy of ipsilateral temporal lobe/hemisphere, and prominence of temporal horn) increases diagnostic confidence. [18] Hippocampal volumetry and T2 relaxometry Increased signal and volume loss can be assessed quantitatively or by visual inspection. With experience, visual inspection of the hippocampus will reliably detect hippocampal asymmetry of more than 20%. A smaller degree of asymmetry is, however, best detected by volumetric quantification. Jackson et al.,[19] have shown that quantitative evaluation of signal is a sensitive (70%) and reliable method for lateralizing HS. Quantitative analysis requires volumetric acquisition sets using either 3D gradient recalled sequence [Figure - 2]a or T2-weighted fast spin echo or turbo spin echo sequence. Quantitative MR volume studies have increased the detection rate and reliability for diagnosing pathologically proved or probable HS, sensitivity 74-96%, and specificity 73-100%. [20],[21] Quantification of hippocampal volumes and signal intensity is used for characterization of cases with bilateral abnormalities, equivocal visual assessment, and research purposes. [22],[23],[24] The advantage of T2 relaxometry, compared with the visual assessment of T2-weighted images, is the quantitative nature of the values obtained. This is particularly useful for patients with bilateral signal intensity increase, for patients with subtle hippocampal signal intensity abnormalities, and for the assessment of subtle signal intensity abnormalities in any other areas. [23] T2 relaxometry is obtained by measuring the decay in signal intensity at different echo times in a series of T2-weighted images through the same slice [Figure - 2]b. Increased T2 relaxation time was predominantly seen in anterior temporal lobe, more pronounced on ipsilateral side, and also on contralateral side. It has been suggested that these abnormalities represent developmental malformations. [25] Histopathologic analysis of the resected tissue showed that increased signal intensity was not associated with dysplasia or gliosis, [26] and it has been suggested that this reflects a persisting developmental stage of the anterior temporal lobe with immature myelin and persistence of immature cells as a consequence of early seizures. T2 relaxometry can lateralize mesial temporal lobe epilepsy even in patients with normal MRI. [27] MR spectroscopy A normal mesial temporal lobe showing high levels of choline presumably reflects a difference in the cellular composition between the allocortex and neocortex. [28] Thus regional metabolic variations must be considered when pathologic conditions involving the mesial temporal lobe are evaluated. There is some evidence to suggest that the distribution of N-acetyl aspartate (NAA) in the hippocampal neurons is not uniform. Mouritzen [29] found an increase in the number of cells from the anterior to the posterior in the pyramidal cells, whereas Babb et al.,[30] did not find statistically significant difference in the number of cells between the posterior and anterior sections. According to Vermathan et al., [31] the anteroposterior difference could be due to fewer neurons in the anterior hippocampus compared with the posterior or due to increasing thickness from the posterior to the anterior leading to different contributions from adjacent tissue. Proton magnetic resonance spectroscopy (1H-MRS) has been used to assess metabolite abnormalities in the seizure focus, and the reduction of NAA is a typical finding [32],[33] [Figure - 3]a-c. In addition, metabolite changes can also be identified outside the seizure focus in patients with HS, reflecting a widespread disorder. [34],[35],[36] MRS not only helps in the diagnosis but also in the prediction of antiepileptic drug response in patients with temporal lobe epilepsy. [37] Diffusion analysis Apparent diffusion coefficient (ADC) analysis gives potential information of both intra- and extracellular spaces and has been shown to help in lateralizing epileptogenic focus in the temporal lobe epilepsy [Figure - 3]d-f. ADC values are significantly higher on the ipsilateral side, and the interictal ADC mapping lateralizes efficiently the lesion side in accordance with the EEG data. [38] Similar significantly increased average ADC values were found in the sclerotic hippocampi compared with controlled subjects in the study by Yoo et al., [39] reflecting neuronal loss, reduction in dendritic branching, and microstructural changes associated with epileptogenesis. Structural neuroimaging in extratemporal epilepsy The etiologic spectrum of extratemporal epilepsy includes the following: disorders of neuronal migration and cortical organization, vascular malformations, and tumors. In the developing countries, infections of the central nervous system account for a significant proportion of the etiologic spectrum. Neocortical gliosis as a sequel to ischemic, traumatic, or infective brain injury may underlie epilepsy. Dysplastic cortex can range from grossly dysmorphic to subtle dysmorphic (with fused gyri and minor irregularities of the cortex-white matter junction) or grossly normal with microscopic abnormalities of lamination. Thus it is essential to analyze HR images in a systematic fashion to pick up these lesions. It is always better to report the MR images on the MRI/PACS workstation rather than on the imaging plates. The cortical gray matter, gray-white junction, gyral and sulcal morphology, and periventricular and subependymal regions must be scrutinized. In children younger than 2 years, the normal myelination pattern must be considered. Imaging sequences are chosen to optimize contrast between gray matter and white matter. In neonates, inversion recovery or spoiled gradient echo T1-weighted sequences and conventional spin echo or RARE T2-weighted sequence allow excellent visualization of the cortex. As the child grows, the white matter begins to myelinate and contrast is lost, first on T1-weighted images (between 3 and 15 months) and then on T2-weighted images (between 8 and 24 months). T2-weighted images are the appropriate sequences for children younger than 8 months and T1-weighted images are the appropriate sequences for children aged between 15 and 30 months. [40] Use of small field-of-view and dedicated phased array surface coils increases the spatial resolution and improves detection and differentiation of focal cortical lesions. [11] Specialized MRI sequences, such as 3D FLAIR [Figure - 4], HR T2, and proton density (PD) techniques should be performed whenever there is a high suspicion of cortical dysplasia, especially when they remain occult on conventional MR protocols. [41] Novel imaging techniques, such as T2 mapping, MRS, MTI, DTI, SWI, double inversion recovery, and HR volumetric techniques, can improve the sensitivity of MRI to localize the anatomic lesion. T2 mapping T2 or transverse relaxation time is sensitive to total amount of water, its distribution, and interaction with microstructural environment. Focally increased T2 signal intensity can be visually appreciated when significant; however, for the detection of occult epileptogenic pathology, quantitative assessment by T2 mapping is more sensitive than qualitative assessment. [42]\ 3D volumetric technique Identification of subtle areas of cortical dysplasia is a time-consuming exercise as it involves analysis of gyrus. For proper analysis, the image must be rotated such that the plane of analysis is perpendicular to, and then parallel to, the section of gyrus being analyzed. 3D Fourier transform volumetric MR examinations with thin partition size appear to be useful in identifying cortical dysplasias in patients with focal epilepsy [Figure - 5]. However, as this is a time-consuming technique, this is likely to be more useful for patients with a seizure focus that is well-localized both by clinical and electrophysiologic criteria. [43] GRE/SWI SWI/T2FNx01GRE sequence should form part of the routine epilepsy protocol as it increases the sensitivity to detect occult calcified lesions [Figure - 6] and also vascular malformations, the substrate for seizures. [44] Diffusion imaging Diffusion is a random process that results from thermal translational motion of molecules. Images that are sensitive to diffusional properties of water can be obtained by incorporating pulsed magnetic field gradients into a standard spin echo sequence. DTI provides a quantitative and informative description of diffusion in anisotropic and heterogenously oriented media, which is impossible to achieve by using diffusion-weighted images or ADCs acquired in 2 or 3 orthogonal directions. A disruption of microstructural environment, such as ischemic injury, gliosis, or cerebral dysgenesis will lead to less ordered arrangement of nerve fiber and reduced anisotropy. These cerebral abnormalities may lead to reduced cell density or expansion of extracellular space, resulting in increased mean diffusivity. [45] Patients with epilepsy and malformations of cortical development (MCD) have been evaluated with DTI and studies reported reduced anisotropy and increased diffusivity in the involved region. [45],[46] This suggests loss of directional organization in combination with preserved cell density [Figure - 7]. In conventional MR-negative cases, white matter integrity abnormalities are seen to extend far beyond the epileptogenic zone. [47] In cases of MCD and extratemporal lesions, reduced anisotropy and increased diffusivity was noted to extend beyond hyperintensity on FLAIR. [48] Magnetization transfer imaging MTI evaluates macromolecular environment. Loss of macromolecules, which is almost exclusively associated with increase in extracellular space and increase in free water, is paralleled by reduction in MTR. MTI analyzed using statistical parametric mapping was sensitive in identifying malformations of cortical development and acquired cerebral lesions. [48] Abnormal MTR was also noted in areas of brain that were normal on visual inspection. [49] Double inversion recovery DIR imaging sequence evaluates white and gray matter compartments separately by applying carefully timed inversion pulses nulling 2 tissues (CSF + gray matter or CSF + white matter) simultaneously providing information on quantity and microstructural environment. Subtle structural abnormalities on DIR have been shown in occult epileptogenic cerebral lesions with negative MRI. [50] MR spectroscopy In contrast to numerous proton MRS studies in temporal lobe epilepsy, there are only a few reports on extratemporal epilepsy. Garcia et al.,[51] reported on the utility of MRS in frontal lobe epilepsy reporting a lateralization in 50% of patients. MRS could be more sensitive in the detection of discrete malformations of cortical development than conventional MRI. [52] It is valuable in the presurgical evaluation of patients without MRI-apparent lesions. The zone of altered metabolism extends beyond the structural and electrographic abnormalities, and may allow detection of pathologies in patients with normal MRI. [52] MRS has the ability to identify small concentrations of neurotransmitters if special editing techniques are used. Measurements of gamma-aminobutyric acid (GABA) have been applied to study the effect of different antiepileptic drugs on the cortex. [53] Contrast-enhanced imaging In cases of late onset epilepsy, contrast should be administered and postcontrast T1-weighted imaging will be useful in demonstrating tumors, vascular malformations, and granulomas. There is no role of contrast-enhanced MRI in the diagnosis of HS. [54] Advanced imaging techniques Advanced imaging techniques, such as tissue classification and segmentation, voxel-based morphometry, texture analysis, cortical and sulcal morphometry, may increase the sensitivity in detection of subtle abnormalities. Computer-aided tissue texture detection technique using complex diffusion approach can help to detect focal cortical dysplasia. [55] Functional neuroimaging in epilepsy Presurgical planning in epilepsy involves identifying eloquent cortex close to the lesion, which if injured during surgery will manifest with neurologic deficit. The goal of presurgical functional imaging is to minimize damage to these functional areas by knowing the location of eloquent cortex. Blood oxygenation level-dependent functional MRI Clinical fMRI is based on blood oxygenation level-dependent (BOLD) contrast. BOLD signal response arises from localized hemodynamic changes induced by regionally increased neuronal activity associated with processing a stimulus or performing a cognitive task defined by the paradigm. BOLD fMRI is a high spatial resolution technique without ionizing radiation that maps physiologic and metabolic consequences of altered electrical activity in the brain. fMRI has the potential to predict the possible deficits in language, and in visual, motor, and sensory functions that would arise from the surgical intervention [Figure - 8]. This helps the treating physician or the surgeon to explain the relative risk of intervention and nonintervention so that a decision about treatment options can be made after considering their costs and benefits. [56] fMRI has been found to be useful in predicting postoperative memory deficit. [57] fMRI not only offers promising noninvasive approach for lateralization of language functions but also more sensitive to involvement of nondominant hemisphere, and thus reduces the need for invasive techniques, such as Wada test and intraoperative cortical stimulation. In selected patients with frequent interictal epileptiform discharges, EEG-correlated fMRI has the potential to identify cortical areas involved in generating the discharges. [57],[58] fMRI studies in focal cortical dysplasia of Taylor's balloon cell type have not shown in situ evidence of electrically inducible function despite their location in otherwise anatomically functional areas, such as the precentral motor cortex. [59],[60] Recent studies have, however, concluded that functional reorganization is unpredictable in cortical malformations. [61] fMRI is a reliable and noninvasive diagnostic tool for presurgical functional assessment without ionizing radiation and offers high spatial resolution. The procedure can easily be performed. However, the patient's cooperation is essential to get quality data and the other limitation is the effect of antiepileptic drugs on BOLD effect. PET and SPECT Functional imaging with SPECT and PET reflects seizure-related changes in cerebral perfusion, glucose metabolism, and neuroreceptor status. In temporal lobe epilepsy, the sensitivity of these methods was shown to be excellent, in particular if a multimodal platform is used, which combines the functional imaging with the additional morphologic information on MRI. However, the sensitivity of PET and SPECT is low in extratemporal lobe epilepsy. [62] Approximately 30% of the patients with temporal lobe epilepsy have a normal MRI scan. [63] In this subgroup of patients, PET studies have shown temporal lobe hypometabolism ipsilateral to ictal onset zone in 87% of the patients. [64] However, in focal epilepsies the reduction in glucose hypometabolism is often widespread and can be even bilateral with most severe hypometabolism in the ictal onset zones. PET interpretation is, however, complicated by functional differences among ictal, postictal, and interictal states. Furthermore, PET images may also reflect altered cerebral functions related to antiepileptic drug therapy. In patients with neuronal migration disorders and subtle cortical dysplasias, PET and SPECT are more sensitive for lesions difficult to detect on MRI [64],[65],[66] [Figure - 9]. The use of perfusion SPECT tracer allows the investigation of ictal onset zone, but the low temporal resolution of ictal perfusion SPECT often results in the detection of both the ictal onset zone as well as the propagation pathways. [62] The usefulness of interictal SPECT for preoperative localization is limited because of its low sensitivity. Ictal SPECT has been shown to have a higher success in lateralizing seizure onset in patients with well-established temporal lobe epilepsy. Extratemporal seizures are frequently associated with multiple areas of increased activity that could be due either to seizure propagation or to individual variability in the baseline patterns of SPECT uptake. The ictal SPECT images should therefore be closely compared with interictal SPECT images. Computer-aided subtraction of the interictal from the ictal SPECT images with subsequent coregistration to MRI (SISCOM) has been shown to overcome many of the limitations associated with the traditional side-by-side inspection of the images. SISCOM improves the sensitivity and the specificity of SPECT in localizing the seizure focus for epilepsy surgery. Concordance between SISCOM localization and site of surgery is predictive of postsurgical improvement in seizure outcome. [67] The highest sensitivity reported with ictal SPECT was 90% for temporal lobe epilepsy and 81% for extratemporal epilepsy. [68] The reported highest sensitivities for interictal-PET, -SPECT, and -qualitative MRI in temporal lobe epilepsy were 84%, 66%, and 55%, respectively. The reported highest sensitivities for interictal-SPECT, -qualitative MRI, and -PET were 60%, 43%, and 33%, respectively. [68] PET or ictal SPECT may be a complementary tool in the presurgical evaluation of patients with medically intractable epilepsy, particularly with negative MRI. [65] Recently, newer techniques of PET imaging with different neuroreceptor ligands, serotonin, GABA, opioid, and dopamine, are under investigation to evaluate the neurochemical basis of epilepsy and the role of these neurotransmitters in the seizure propagation. Conclusion MRI forms the mainstay for structural and functional neuroimaging in patients with epilepsy [Figure - 10]. With increasing availability of newer techniques and HR sequences, the sensitivity and specificity of detecting epileptogenic lesion on MRI has increased. The MRI demonstration of a lesion very much helps in further presurgical evaluation. In patients with negative MRI, PET and SPECT may be used as complimentary tools in the presurgical workup. In the recent years, advances in neuroimaging have helped to understand the pathophysiology of epilepsy better and also to prognosticate the outcome of medical and surgical treatments. The advancements have also provided noninvasive tools to detect the epileptogenic focus. References
Copyright 2010 - Neurology India The following images related to this document are available:Photo images[ni10098f2.jpg] [ni10098f7.jpg] [ni10098f6.jpg] [ni10098f1.jpg] [ni10098f10.jpg] [ni10098f3.jpg] [ni10098f8.jpg] [ni10098f4.jpg] [ni10098f5.jpg] [ni10098f9.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}