 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 58, No. 3, May-June, 2010, pp. 377-383 Original Article Magnetic resonance imaging evaluation of subarachnoid hemorrhage in rats and the effects of intracisternal injection of papaverine and nitroglycerine in the management of cerebral vasospasm Shashank R Ramdurg1, Ashish Suri1, Deepak Gupta1, Sujeet Mewar2, Uma Sharma2, NR Jagannathan2, Bhavani S Sharma1 1 Department of Neurosurgery, All India Institute of Medical Sciences, New Delhi, India Date of Acceptance: 10-Jun-2010 Code Number: ni10100 PMID: 20644264 Abstract Background : Cerebral vasospasm is a major cause of morbidity and mortality after subarachnoid hemorrhage (SAH). It usually occurs about 3-9 days after SAH. The pathogenesis involves the release of endogenous spasmogens. Though various treatment modalities are available, none are really effective.Aims and Objectives : The aim of the study was to develop an effective animal model for the study of SAH and vasospasm as well as to study the efficacy of vasodilators, namely nitroglycerine and papaverine, on SAH-induced vasospasm using magnetic resonance angiography. Materials and Methods : Fifteen Wistar albino rats, weighing around 150-200 gm were used for the study. Five rats served as controls of SAH-induced vasospasm, while five rats each were used to study the efficacy of intracisternal injection of papaverine or nitroglycerine. Results : Rats demonstrate vasospasm in a manner similar to humans. The maximal vasospasm is seen in the basilar artery. Statistical analysis demonstrates an improvement in vasospasm after instillation of intracisternal papaverine at the end of 2 hours in basilar and left internal cerebral artery. However, nitroglycerine does not produce any significant amelioration of vasospasm. Thus, it can be deduced that the pathogenesis of the vasospasm is more due to the action of cGMPase enzyme rather than inhibition of nitric oxide (NO) synthetase by the spasmogens. The present study is the first study in the English literature to compare the effects of single bolus doses of nitroglycerine and papaverine using magnetic resonance angiography. Conclusion : Rats can be used to create an effective model for SAH-induced vasospasm as the pattern resembles human SAH. Papaverine is an effective drug for ameliorating SAH-induced vasospasm. Short-acting NO donors are not as effective in ameliorating vasospasm. Keywords: Animal model, intracisternal, papaverine, subarachnoid hemorrhage, vasospasm
The incidence of subarachnoid hemorrhage (SAH) is estimated to be around 6-8 per 1 00 000 person-years. One quarter of patients die within the first 24 hours. Mortality is estimated to be around 45% at 30 days. [1] Histopathological studies of brains of patients who died shortly after SAH show global ischemic change, the cause of which is unclear. Cerebral vasospasm is a major cause of morbidity and mortality after SAH. This usually occurs about 3-9 days after aneurysmal SAH. Some form of ischemic deficit develop in 27%-38% of patients due to cerebral vasospasm. [1] The pathogenesis of vasospasm involves multiple endogenous spasmogens, including oxyhemoglobin and endothelin. These are believed to inhibit nitric oxide (NO) synthetase and thus reduce the levels of endogenous vasodilator, thereby producing vasoconstriction. [2],[3] Various studies have demonstrated the efficacy of long-acting NO donors and intrathecal infusion of glycerol trinitrate, supporting this hypothesis. [4],[5] However, there are other studies that have failed to demonstrate the efficacy of exogenously administered NO donors. [6] Thus, the question of whether NO synthetase inhibition is the sole mechanism for vasospasm has to be answered. Many studies have demonstrated the efficacy of phosphodiesterase inhibitors like papaverine, suggesting a role of destructive enzymes like cGMPase in the pathogenesis of vasospasm. [7] Various strategies have evolved for the treatment of vasospasm; [2] however, the magical bullet remains elusive. Most of the drugs utilized are used intravenously. The time of action and the concentration reaching the affected vessels hence remains a question to be answered. In this study, we adopt rat experimental models for the study of SAH-induced vasospasm. The aim of the study is to investigate the pathogenesis of vasospasm after SAH using magnetic resonance angiography (MRA). Use of MRA enables in vivo measurement of vessel diameter. The study was designed to test whether short-acting NO donors have a role in ameliorating vasospasm and to compare the efficacy of NO donors with that of phosphodiesterase inhibitors using short bolus doses of the drugs, thereby providing an insight to the pathogenesis of vasospasm. This is the first study to use MRA to compare the efficacy of single-bolus doses of a short-acting NO donor and a phosphodiesterase inhibitor. Aims and objectives The study was designed to:
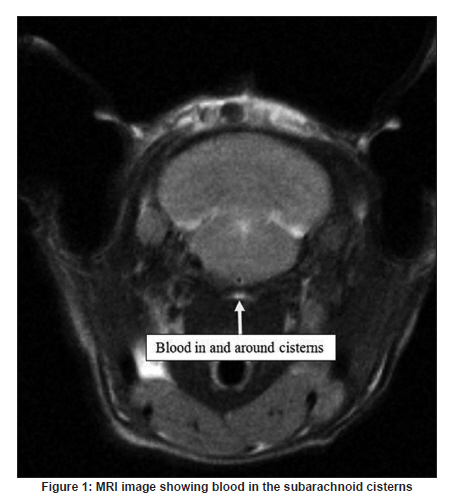
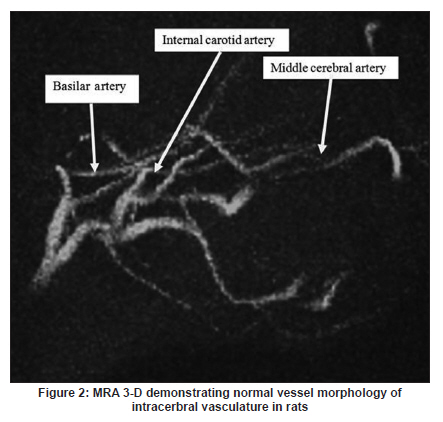
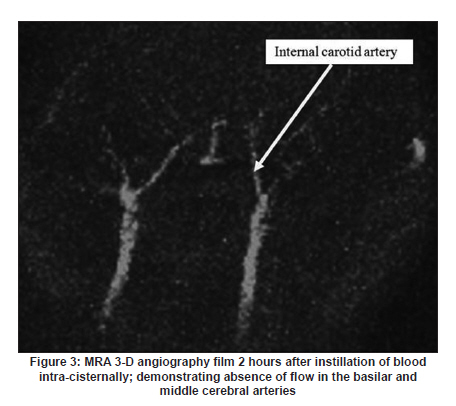
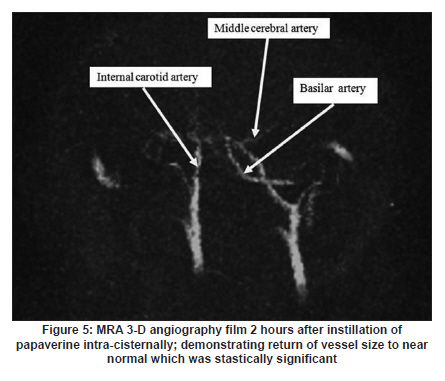
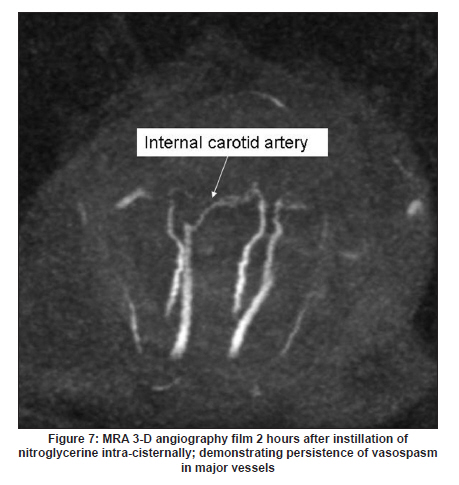
Materials and Methods Animal preparation Institute Animal Ethics Committee approval was obtained for the study. The study included a total of 15 Wistar albino rats, weighing around 150-200 gm each. Five rats were used to demonstrate the effects of SAH in rats. The animals were anesthetized by intraperitoneal injection of chloral hydrate. They were allowed to breathe spontaneously. A preprocedural MRI/MRA was performed using a 4.7-Tesla animal MRI machine to ascertain the original vessel size. The diameters were measured by software provided by the manufacturer (Biospec Bruker, Switzerland). A 24-gauge needle was used to aspirate autologous blood from the tail vein. The rats were then placed in a prone position with the head flexed. The atlanto-occipital membrane was exposed through a midline suboccipital incision. This was then punctured with a 27-gauge needle and 0.1 mL of cerebrospinal fluid (CSF) was aspirated. Following this, 0.1 mL of autologous blood from the rat tail was injected in the control animals. MRI and MRA were repeated after 2 hours and after 48 hours to look for vasospasm. Study group 1 Five rats were used to study the efficacy of papaverine in reducing vasospasm. SAH was induced in these rats as explained above. Following 2 hours of instillation of autologous blood (similar to the control group), MRI was performed after 1 hour (before full effect of vasospasm). After MRI, 0.1 mg/kg body weight of intracisternal papaverine was instilled. MRI and MRA were repeated after 1 hour (i.e., a total of 2 hours post SAH) and 48 hours, respectively, and the vessel diameters were measured. Study group 2 Five rats were studied for the efficacy of intracisternal glycerol trinitrate in the dose of 0.1 mg/kg body weight. The steps followed were the same as that in study group 1. MRI/MRA parameters MRI and MRA were performed using a 4.7-Tesla animal scanner (Bruker, Switzerland). Time of flight MRA was performed using 3D gradient-echo sequences with TR/TE = 15/2.8 ms; flip angle 20°; FOV 4 Χ 4 Χ 2 cm3; matrix 256 Χ 256 Χ 128. T2-weighted images were obtained using a multi-slice, multi-echo CPMG sequence: TR = 3000 ms, TE = 56 ms; 14 echoes; FOV 4 Χ 4 cm 2 ; slice thickness 2 mm; inter-slice distance 2 mm; matrix 256 Χ 256. Statistical analysis Analysis was performed using analysis of covariance (ANCOVA) test/post hoc Tukey test. Statistical significance was taken at P<.05. Each of the five vessels were tested regarding degree of vasospasm and the effect of drugs. Results There was one death in each of the groups within 2 hours of SAH. Additional deaths - two in the control group and one each in study groups 1 and 2 - occurred after 24 hours Each of the rats in the SAH group was studied using T2W imaging and 3-D MRA; imaging was done pre-SAH, 2 hours post-SAH, and on the second day post-SAH. In study groups 1 and 2, the images were obtained pre-SAH as well as twice post-SAH: 2 hours after instillation of papaverine/nitroglycerine and 2 days after instillation of the respective drug. The vessels studied were the basilar arteries, carotid arteries, and the middle cerebral arteries [Figure - 1], [Figure - 2], [Figure - 3], [Figure - 4], [Figure - 5], [Figure - 6], [Figure - 7], [Figure - 8]. SAH group It was observed that the vessels affected most were the basilar arteries followed by the middle cerebral arteries [Figure - 3] and [Figure - 4]. Most parts of basilar arteries were not visible after SAH at the end of the second hour, the reduction in size thus being 100%. Three of the four rats demonstrated a 100% reduction in the size of middle cerebral arteries bilaterally. The internal carotid arteries were the least affected. The discrepancy in the diameters between the right and left sides was possibly because the direction in which the blood was injected caused a difference in the concentrations in the two sides. After 2 days, the effect of vasospasm was still present, as evidenced by the persistence of reduction in the vessel size [Figure - 4]. Only two rats survived - a mortality of 50%. Papaverine study group The post-SAH findings were similar to that observed in the SAH group. However, as the scans were performed at 1 hour, before maximal vasospasm could set in, the vessel diameters were comparatively unaffected. The basilar artery however continued to demonstrate 100% reduction and was not visible in most parts in all the rats. Three of the four middle cerebral arteries demonstrated 100% reduction in vessel size, while the carotid arteries showed less change in vessel diameter [Figure - 5] and [Figure - 6]. Post papaverine injection, all the vessels substantially increased in size, with the maximum effect being seen again in the basilar and the middle cerebral arteries. These vessels demonstrated significant increase in vessel size, reaching almost 60-180% of original lumen size at the end of 2 hours. Though there was some improvement in the vessel caliber at the end of 48 hours, this was not statistically significant. Nitroglycerine study group The effect of glycerol trinitrate in study group 2 was not marked as compared to the papaverine group. No significant vasodilatation was seen in any of the vessels at 2 hours and 48 hours [Figure - 7] and [Figure - 8]. There was a decrease in size in the basilar and the middle cerebral vessels at 2 hours and 48 hours despite the instillation of nitroglycerine. Some improvement in the diameters of the internal carotid vessels was seen at 2 hours; however, this was not statistically significant. Statistical analysis Significant improvement in vasospasm was seen only with papaverine at 2 hours in the basilar artery and left internal carotid artery (P=.08, P=.017). However, the effect was not sustained at 48 hours (P=.89, P=.29). No statistically significant improvement was seen in the other vessels with papaverine. No significant improvement was seen with nitroglycerine in any of the vessels either at 2 hours or 48 hours [Table - 1]. Discussion Cerebral vasospasm is an angiographically demonstrable narrowing of intracerebral arteries. It can be asymptomatic or clinically symptomatic, when there may be severe neurological deficits or even death. [1] After the onset of SAH, an immediate event of acute global ischemia is encountered. This is then followed by the more delayed vasospasm, which is responsible for the neurological deterioration and death. Cerebral vasospasm is now the leading cause of permanent disability and death in patients with ruptured cerebral aneurysm. [2] In 1928, Bagley systematically studied the effects of repeated hemorrhages in the subarachnoid space. [3] Jackson termed the condition as 'aseptic hemogenic meningitis.' He identified oxyhemoglobin as one of the important mediators of vasospasm. [8] SAH models in experimental animals have been used to simulate human SAH after aneurysmal rupture. Both craniotomy and non-craniotomy models are used. Non-craniotomy models have the added advantage of demonstrating coexistent rise in intracranial pressure. It can be either induced by the endovascular suture technique or by injecting blood into the subarachnoid space. The latter is an easier and convenient technique, with less fatality rate as compared to the former. Hence we preferred this model of SAH in our experimental models. [3] Rats demonstrate a pattern of vasospasm similar to humans. The duration of this vasospasm is for around 3 days. [9] A similar biphasic pattern of vasoconstriction has been demonstrated in dogs [10] as well as in primates. [11] One of the contributory factors for immediate vasoconstriction is thought to be arginine vasopressin. [12] Various studies have tried to elucidate the causes of these events. [13] Oxyhemoglobin and deoxyhemoglobin are the principal pathogenic substrates. However, the mechanisms involved in the genesis of vasospasm have remained elusive. [1] The role of NO synthetase inhibitors has been highlighted in most of the studies. However, our study shows that phosphodiesterase inhibitors are more efficacious than NO donors. Thus, the destructive enzyme cGMPase is more important than NO synthetase in the genesis of vasospasm. The pathogenesis of delayed vasospasm is said to be multifactorial. It involves changes in smooth muscle cells (proliferation and/or necrosis), [14],[15] and endothelial cells (damage and apoptosis). [16] a variety of molecular mediators [17],[18] and proinflammatory mediators are also involved. [19] The degree of vasospasm, in turn, was found to be proportional to the amount of blood injected. [1] Acute cerebral ischemia after SAH involves acute vasoconstriction, elevation of intracranial pressure within minutes, and attendant reduction in cerebral perfusion pressure. [20] Cerebral metabolic rate and spontaneous electrical activity both decrease in the early phases of SAH. Severe SAH is also associated with loss of autoregulation and uncoupling of metabolism and cerebral blood flow. [21] Microvascular aggregation of red blood cells leading to a no-reflow phenomenon has also been proposed as a mechanism of acute ischemia after SAH. [22] Techniques to quantify vessel diameter in small animals is a challenging task. Previous studies have used Doppler ultrasound to quantify vasospasm and hence are subjective. Performance of angiography is technically challenging. Therefore we used MRA to quantitatively study the vessel diameters, document vasospasm, and study the effect of drugs. MR techniques can measure cerebrovascular alterations and ischemic lesion development after SAH in the rats. There is an increase of the ischemic lesion between day 0 and day 2 after SAH, and the simultaneous vasoconstriction suggests that delayed cerebral ischemia related to vasospasm occurs in rats after SAH. [23] The attenuation of the acute vasoconstriction by early treatment with pharmacological agents may prove beneficial in the management of both the initial phase of acute vasoconstriction and in delayed ischemia. [24] Though various treatments have been tried, the 'magic bullet' still remains elusive. Cardiopulmonary stabilization, analgo-sedation, and extraventricular drainage procedures to reduce intracranial pressure remain the initial measures in the management of the acute phase of SAH. [25] 'Triple H' therapy - i.e., hemodilution, hypertension, and hypervolemia, is the mainstay of management of delayed cerebral ischemia following clipping of an aneurysm. Various drugs have been used in the management of SAH to improve the cerebral perfusion pressure. They are delivered either by the oral route or intra-arterially. However, therapeutic concentrations are often not achieved or take a longer duration to do so. Intracisternal delivery of these drugs would achieve therapeutic concentrations within a short period of time. Papaverine is a commonly used drug in the treatment of SAH. Its intra-arterial use has been well studied. By inhibiting phosphodiesterase enzyme, it increases the levels of NO and causes vasodilatation. [25] The dose used is 0.1 mg/kg body weight. Experimental studies using intra-arterial infusions of papaverine have demonstrated its efficacy in past. A study done by Hon Man Liu et al. demonstrated its efficacy both by intra-arterial and intracisternal routes. [7] Our study demonstrated the efficacy intracisternal instillation of papaverine in ameliorating vasospasm. The effect can be seen even at the end of 2 days, though at reduced levels; this emphasizes the importance of early treatment of vasospasm, before full-blown vasospasm can set in. Repeated doses of papaverine could be helpful in sustaining the CSF levels of papaverine. The mortality in the papaverine-treated rats was also lower than in control group. The authors, on the basis of this experiment also suggest that topical papaverine could be used in the management of vasospasm in aneurysm surgeries. The rats in our study were monitored for their respiratory and cardiac status during the experiment and the parameters were found to be stable. However, a larger number of subjects would be required to ascertain the complications that would arise from the multiple intrathecal injections of papaverine. NO synthetase has been postulated to be one of the main mediators in the development of vasospasm. Studies using long-lasting NO donors and continuous infusions of glycerol nitrate have supported this hypothesis. [4],[5] However, other studies have refuted this claim by demonstrating that other NO donors, e.g., sodium nitroprusside, do not ameliorate SAH-induced vasospasm. [6] In our study, a short bolus dose of glycerol trinitrate failed to ameliorate SAH-induced vasospasm. Thus, activation of destructive enzymes like cGMPase probably has a greater role in the pathogenesis of vasospasm than the inhibition of NO synthetase. Previous studies have used continuous infusions/longer-acting NO donors, thus providing a constant source of NO for vasodilatation despite degradation. Moreover, the use of continuous intrathecal infusions of NO donors would not be practical in clinical settings. Conclusion Vasospasm is an important cause of mortality in patients with SAH. This experiment demonstrates an effective SAH model for rats and the use of MRI and MRA for demonstration of SAH-induced vasospasm. This study demonstrates the efficacy of papaverine in the treatment of SAH-induced vasospasm, especially when the drug is given intracisternally. Another important implication is the possibility of topical application of papaverine in the management of vasospasm during aneurysm and other surgeries. Short-acting NO donors given in bolus doses, however, have no role in the management of vasospasm. Thus, it appears that destructive enzymes like cGMPase have a greater role in the pathogenesis of SAH-induced vasospasm than inhibition of NO synthetase. References
Copyright 2010 - Neurology India The following images related to this document are available:Photo images[ni10100f1.jpg] [ni10100f3.jpg] [ni10100f2.jpg] [ni10100f5.jpg] [ni10100f6.jpg] [ni10100f8.jpg] [ni10100f4.jpg] [ni10100t1.jpg] [ni10100f7.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}