 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
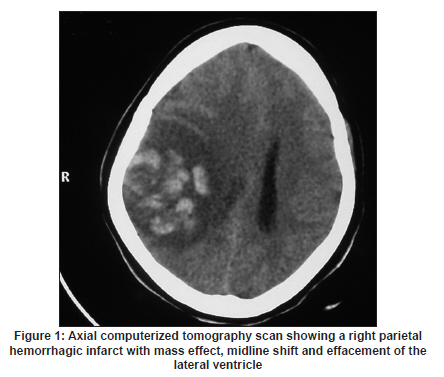
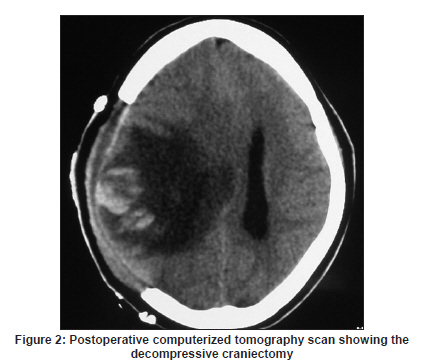
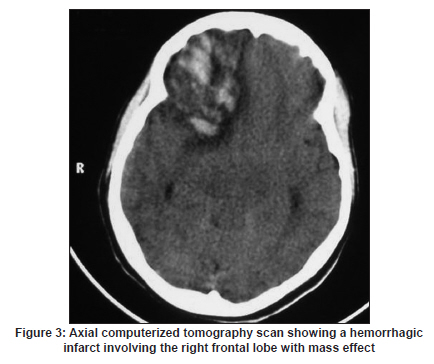
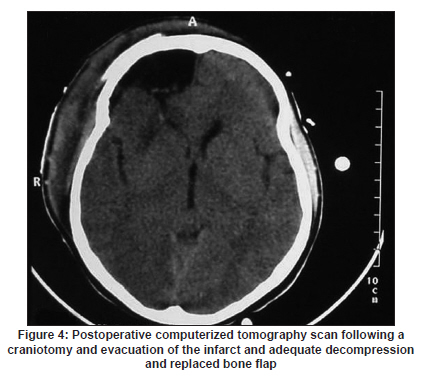
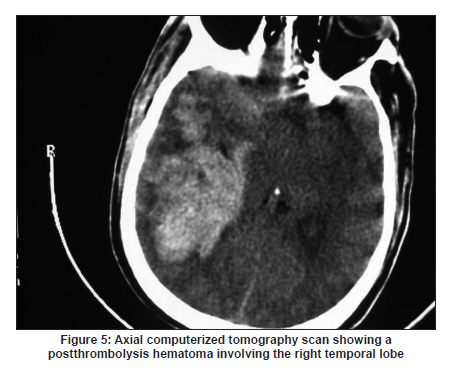
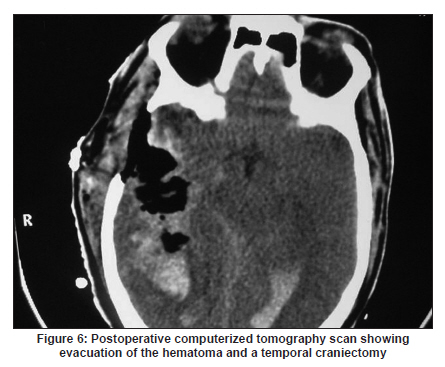
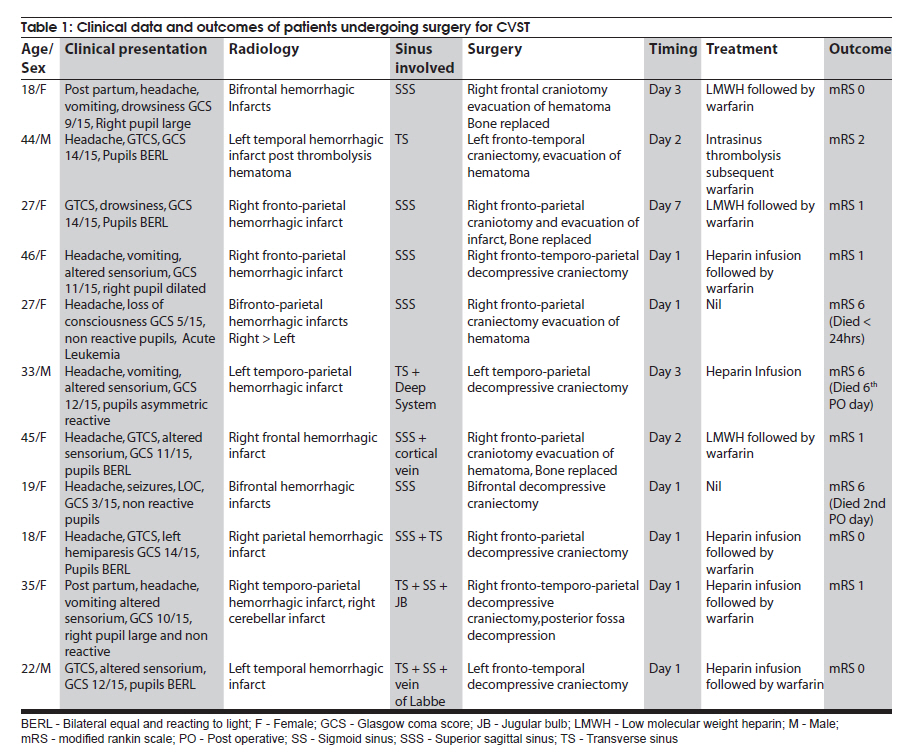
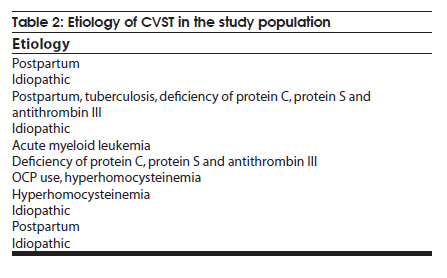
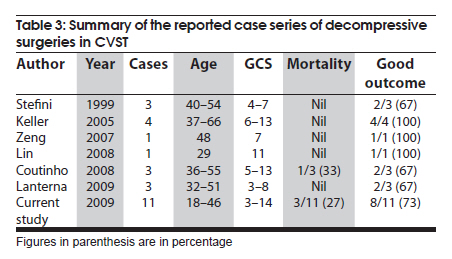
Neurology India, Vol. 58, No. 3, May-June, 2010, pp. 392-397 Original Article Decompressive surgery for severe cerebral venous sinus thrombosis Rahul Lath, Sudhir Kumar, Rajesh Reddy, Gnana Ratnam Boola, Amitava Ray, Subhashini Prabhakar, Alok Ranjan Stroke Unit, Department of Neurosciences, Apollo Hospitals, Hyderabad - 500 033, Andhra Pradesh, India Date of Acceptance: 21-Sep-2009 Code Number: ni10102 PMID: 20644266 Abstract Background : Cerebral venous sinus thrombosis (CVST) is one of the common causes of stroke in young people. Mortality in CVST, in addition to progressive thrombosis, is related to elevated intracranial pressure causing transtentorial herniation. The role of decompressive surgery in CVST is not well established. Keywords: Cerebral venous sinus thrombosis, decompressive craniectomy, functional outcome, mortality Introduction Cerebral venous sinus thrombosis (CVST) is a disorder of varied etiology, with an annual incidence of three to four cases per 1 million population. [1] CVST accounts for 10-20% of the etiology of young strokes in India. [2],[3] The therapeutic options in CVST include antithrombotic therapy with conventional heparin, low molecular weight heparin (LMWH) or oral anticoagulants and intravenous or intrasinus local thrombolysis. [1],[3],[4] Anti-epileptic drugs and anti-edema agents are used as per the clinical situation. Poor outcome in the International study on Cerebral Vein and Dural Sinus Thrombosis (ISCVT) was 13.6%. [5] The factors predicting an unfavorable outcome included male sex, age >37 years, coma, mental status disorder, intracranial hemorrhage on admission, thrombosis of the deep venous system, central nervous system (CNS) infection and cancer. During the acute phase of CVST, 4.3% of the patients died and 3.4% died within 30 days from symptom onset. [6] The main cause of death in the acute phase was neurological deterioration secondary to transtentorial herniation. Severe increase in intracranial pressure (ICP) in the acute phase of CVST is usually treated medically, often without success. There have been a few reports of favorable outcome following decompressive surgery in the acute phase of CVST. [7],[8],[9],[10],[11] We report our experience with decompressive surgery in CVST. Materials and Methods The medical records of patients admitted with the diagnosis of CVST between December 2003 and July 2009 were reviewed. Diagnosis of CVST The diagnosis of CVST was made on the basis of presenting clinical features and radiological findings, computerized tomography (CT) scan and/or magnetic resonance (MR) scan with venography. Medical management Patients were admitted to the intensive care unit (ICU). All patients had a detailed neurological evaluation and assessment of sensorium by Glasgow Coma Scale (GCS). All patients were initially treated with low molecular-weight heparin (LMWH) or conventional heparin infusion. Partial thromboplastin time (PTT) monitoring was done to adjust the dose of conventional heparin. Anti-epileptic drugs and anti-edema agents were used as deemed necessary. Etiological work-up included pretreatment thombophilia screening (Protein S, Protein C, Antithrombin III), serum homocysteine and antiphospholipid antibodies. Indications for surgery Indications for surgery included: a low GCS (8 or less) at admission with large infarct on the CT/MRI scan; significant mass effect and midline shift on CT/MRI scan; clinical and radiological signs of transtentorial herniation; deterioration in the sensorium despite anti-edema measures; and post intra-sinus thrombolysis hematoma. Surgical procedure and postoperative management The site and size of decompressive craniectomy was based on the location and size of the venous infarct [Figure - 1] and [Figure - 2]. A bone flap larger than the venous infarct was made and the dura was widely opened and patched with the pericranium. The wound was closed in layers over a drain. In three patients, the bone flap was replaced after evacuation of the hemorrhagic infarct in the noneloquent regions [Figure - 3] and [Figure - 4]. One patient with postthrombolysis hematoma had removal of the temporal hematoma [Figure - 5] and [Figure - 6]. Postoperatively, patients were monitored in the ICU and were mechanically ventilated in most cases. Twelve hours after surgery, anticoagulation with either heparin infusion or LMWH was resumed and subsequently changed to oral anticoagulation with warfarin. Oral anticoagulation was continued for at least 6 months. Patients with a craniectomy had a cranioplasty performed 3-6 months following the decompressive surgery. Assessment of outcome Patients were followed-up for at least 6 months. Functional outcome among survivors was assessed using the modified Rankin scale (mRS). [12] Mortality rate was also calculated. Results Patient characteristics One hundred and six patients were admitted with the diagnosis of CVST during the study period. Eleven patients (10%) underwent decompressive surgery, while three patients (2.8%) underwent a lumbar-peritoneal shunt in the acute phase of CVST. The clinical details of these 11 patients are summarized in [Table - 1] and [Table - 2]. The mean was 30.4 years (range 18-46 years) and the female (73%) was predominant gender. Indications for surgery Indications for surgery included: a low GCS at admission with large infarct on the CT scan in two; mass effect and midline shift in two; clinical and radiological signs of transtentorial herniation in two; deterioration in the sensorium despite best medical management in four; and postthrombolysis haematoma in one. Six patients (55%) underwent decompressive surgery within 24 h of admission. Three patients who underwent a shunt surgery had normal sensorium but developed progressive deterioration in visual acuity with severe papilledema, despite anticoagulation and anti-edema treatment. Outcome Three patients (27%) died following the decompressive surgery (one each on the first, second and sixth postoperative days). Of the three patients who died, two had a low GCS and bilaterally nonreactive pupils at admission, while one patient had a normal sensorium but continued to deteriorate in spite of anticoagulation and anti-edema measures. This patient continued to deteriorate even after a decompressive craniectomy. He had features of deep venous system involvement. Survivors were followed for a mean period of 7.4 months (range 6-10 months). At follow-up, eight patients (73%) had a good functional outcome (mRS 0-2). No surgery-related complications were noted. Discussion Decompressive hemicraniectomy for malignant arterial infarctions is now well accepted. It reduces mortality and results in better functional outcome. [13],[14],[15] The mortality from CVST has been variously reported and range from 0 to 36%, it was 4.3% in the the ISCVT. [6] The cause of death in the majority of these patients was neurological deterioration secondary to transtentorial herniation. The investigators involved in this study have suggested that decompressive craniectomy should be considered in patients with progressive transtentorial herniation in order to decrease the mortality rates. [5],[6] Medical management of raised ICP consists of mannitol, steroids and hyperventilation. Mannitol has a rapid onset of action and is very effective in reducing ICP. Thus, mannitol is often the treatment of choice in a patient with CVST with features of elevated ICP. However, mannitol has several limitations. Its use is limited in the setting of hypotension, renal failure and cardiac failure. Further, there is the risk of rebound increase in ICP following discontinuing mannitol. Osmotic agents might be harmful in patients with venous outflow obstruction because these agents may not be quickly eliminated from intracerebral circulation as in the case of other disease states. [4] Corticosteroids efficacy is unproven and are harmful as they promote the thrombotic process. [4] A recent study had shown that steroids in the acute phase of CVST were not useful and were detrimental in patients without parenchymal cerebral lesions. [16] In patients with massive space-occupying venous infarct, these management strategies may not be effective. There are no randomized trials comparing decompressive surgery with best medical management in CVST. However, it is evident that in severe cases with life-threatening unilateral large hemorrhagic infarct, decompressive surgery may be the only life saving option. [4] In view of the relatively low incidence of CVST and fewer number of patients requiring surgery (1.4% in ISCVT), a randomized trial would be difficult. A prospective multicenter study, ISCVT-2, is underway and the data following decompressive surgery in CVST are being collected. [17] In the pre-CT/MRI scan era, the largest number (34 patients) of decompressive surgeries in CVST was reported by Nagpal in 1983. [18] The preoperative neurological status and outcome assessment have not been mentioned. The author has stated that 56% of the patients undergoing surgery survived while 44% died. The outcomes of decompressive surgery in CVST in the post-CT/MRI scan era are summarized in [Table - 3]. It is evident from these reports that decompressive surgery in CVST has survival benefit and this is in spite of a poor preoperative neurological status. This survival benefit was also seen in patients with bilateral nonreactive pupils. [8] However, two of our patients with bilateral nonreactive pupils did not survive. One them was a case of leukemia. We feel that decompressive craniectomy should be offered before pupillary changes. Decompressive craniectomy may be beneficial in patients who develop hematoma following thrombolysis therapy. Characteristics of patients who may benefit or who may not benefit from decompressive surgery are given in [Table - 4]. Of the 106 patients with CVST, three patients had lumbar-peritoneal shunt (2.8%) surgery in the acute phase of illness, the indications were deterioration in vision and severe papilledema, despite adequte anticoagulation. None of them had significant venous infarct and altered mental status. Vision improved in all the three patients following the shunt procedure. Shunt surgery was the treatment in 1.6% of the patients in the ISCVT study. [5],[6] A lumbar-peritoneal shunt would be indicated in patients with visual deterioration in the acute phase. [19] Shunts may be required in the chronic phase of illness in those patients who develop features of elevated intracranial hypertension. Surgical procedures like open thrombectomy and venous bypass may not be of much significance in the treatment of CVST in view of the endovascular modalities currently available. [20],[21] References
Copyright 2010 - Neurology India The following images related to this document are available:Photo images[ni10102t1.jpg] [ni10102t2.jpg] [ni10102f5.jpg] [ni10102f6.jpg] [ni10102t4.jpg] [ni10102f3.jpg] [ni10102f1.jpg] [ni10102t3.jpg] [ni10102f2.jpg] [ni10102f4.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}