 |
search
for |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
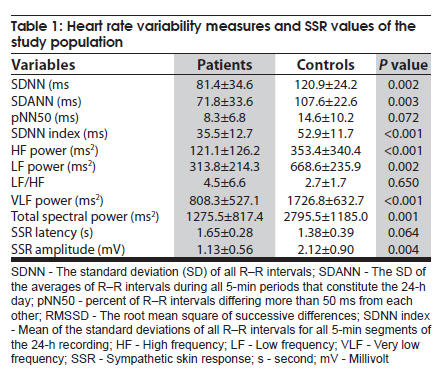
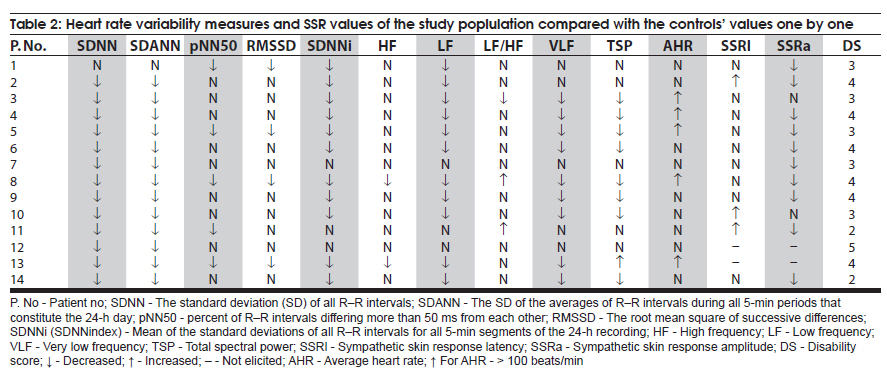
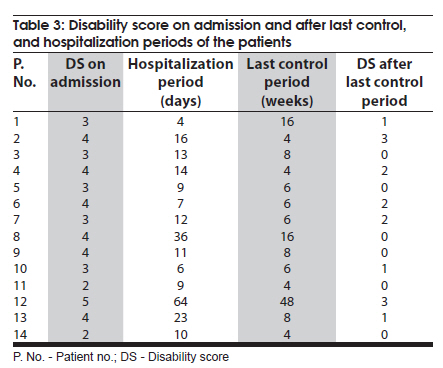
Neurology India, Vol. 58, No. 3, May-June, 2010, pp. 398-402 Original Article Selective autonomic screening in Guillain-Barré syndrome Deniz Yerdelen1, Tansel Erol2, Mehmet Karatas1 1 Department of Neurology, Baskent University Faculty of Medicine, Adana Teaching and Research Center, Dadaloglu mah. 39 sok. Yüregir-Adana- Posta kodu: 01250, Turkey Date of Acceptance: 01-Feb-2010 Code Number: ni10103 PMID: 20644267 Abstract Background : Autonomic dysfunction is a common and important complication in Guillain-Barre syndrome (GBS) and may be the cause of significant morbidity or death. Keywords: Guillain-Barre syndrome, autonomic function, sympathetic skin response, 24-h heart rate power spectrum Introduction Guillain-Barré syndrome (GBS) is an inflammatory demyelinating disorder of the peripheral nervous system, clinically characterized by acute flaccid paresis, areflexia and protein-cytologic dissociation in the cerebrospinal fluid. [1] Autonomic dysfunction is a common and important complication in GBS and occurs in approximately two-thirds of patients. [2] Besides motor and sensory deficits, GBS is often associated with a variety of autonomic involvements including cardiovascular, vasomotor, or sudomotor dysfunctions in both the sympathetic and parasympathetic systems. Signs of sympathetic and parasympathetic failure may be present, as well as overactivity of the sympathetic and parasympathetic nervous system. Autonomic function tests applied in GBS patients have shown the necessity of monitoring autonomic disturbances in every patient with GBS, with or without autonomic dysfunction signs and symptoms. [3],[4] Sympathetic skin response (SSR) is a noninvasive method that can be used easily to evaluate autonomic dysfunction. It involves a recordable skin potential change following the application of an internal or external stimulus. [5] Although it has been used in a variety of clinical settings to evaluate sudomotor sympathetic function, we found only one study associated with SSR in GBS in PubMed. [6] The analysis of variations in the heart rate has been used to determine the balance between sympathetic and vagal nerve activities in the heart. [7] There have been only a few studies which used a 24-hour (24-h) heart rate power spectrum for evaluation of autonomic dysfunction in GBS. Their results indicated that 24-h heart rate power spectrum is a powerful predictor of serious autonomic complications in patients with GBS, and may help to identify patients at risk of potentially life-threatening arrhythmias. [8],[9] In this report, SSR, time and frequency domain analysis of heart rate variability (HRV) gathered from a 24-h electrocardiogram recording have been studied in patients with GBS to show the possible autonomic involvement. Materials and Methods Patients Fourteen GBS patients [six women and eight men; 37.1 ± 16.2 (mean ± SD) years old] were studied. Patients gave informed consent for the examinations. The patients who had preexisting diseases that may cause autonomic involvement were excluded. None of the patients had hypertension, arrhythmia, ischemic or other heart diseases, chronic obstructive airway disease, diabetes mellitus, hypothyroidism, alcoholism or central nervous system disease. So, they didn't take any specific therapy that could affect the autonomic tests. Seven patients had an upper respiratory tract infection with an interval ranging from 5 to 10 days before the onset of neuropathy. Two patients were pregnant with gestational ages of seven and eight months, respectively. Thirteen patients consulted our clinic within 6.5 ± 3.7 days from onset (ranging from 2 to 15 days). One patient was admitted to the clinic in the second month of the disease while he was in the convalescence state. Based on the initial electrophysiological findings, 13 patients had acute inflammatory demyelinating polyneuropathy (AIDP) and one had acute motor axonal neuropathy (AMAN). The patients' disability was graded on a scale modified from Hughes et al. with [10] : 0= normal functional state without neurological deficits; 1= minor signs or symptoms but being able to perform manual work; 2= able to walk 5 m or more without assistance; 3= able to walk 5 m or more with assistance; 4= chair or bed-bound; 5= requiring mechanical ventilation, and 6= death. Seven patients were treated with plasmapheresis, three with intravenous immunoglobulin, and three with a combination of both. One patient who was in the convalescence state of the disease received no specific therapy. Only one patient required mechanical ventilation for 30 days. None died during the hospitalization period. Controls Control values for SSR were elicited from electro-physiology laboratory normal values of the neurology department including 11 healthy subjects, four men and seven women, aged 35.0 ± 6.7 years without any signs or symptoms of autonomic dysfunction. Control values for HRV measurements were provided from normal data of the cardiology department including 14 healthy subjects, seven men and seven women, aged 36.6±9.4 years without any signs or symptoms of autonomic dysfunction. Autonomic function tests For the palmar SSR, surface electrodes were used with the active recording electrode placed on the palm of the hand and the reference electrode located at the wrist on the dorsum of the hand. SSR parameter included the latency to the onset of depolarization which was indicated by the first continuous deflection from the baseline. The amplitude was measured from peak to peak. Four successive SSRs were induced by unexpected acoustic stimuli, pinprick, touching and median nerve electrical stimulation at 30 milliampere stimulus intensity. The stimulating electrodes were placed over the contralateral median nerve. The mean of these four latencies and amplitudes were accepted as the valid value. The study used an electromyography machine with the filter settings for the low frequency at 0.5 hertz (Hz), and the high frequency at 500 Hz. The sweep speed was set at 300-500 ms per division. Examinations were performed in a quiet room and skin temperature was maintained at >32ΊC. The subjects were kept awake and relaxed. The parameters of HRV were gathered from a 24-h electrocardiogram recording. All recordings were analyzed using the Cardioscan Suprima 10 software system (Energy-Lab Technologies GmbH, Hamburg, Germany) with DMS 300 digital Holter recorder (The V Bravo Company, CA, USA) with manual correction of artifacts. HRV was assessed in two ways: (1) time domain analysis and (2) frequency domain analysis. The following time domain indexes were obtained: (1) the standard deviation (SD) of all R-R intervals (SDNN), (2) the SD of the averages of R-R intervals during all 5-min periods that constitute the 24-h day (SDANN), (3) percent of R-R intervals differing more than 50 ms from each other (pNN50), (4) the root mean square of successive differences (RMSSD), and (5) mean of the standard deviations of all R-R intervals for all 5-min segments of the 24-h recording (SDNN index). In the frequency domain analysis; (1) very low frequency (VLF) power, defined as the power ≤ 0.04 Hz, (2) low frequency (LF) power, the power between the 0.04 to 0.15 Hz, (3) high frequency (HF) power, the power between the 0.15 and 0.40 Hz and (4) total spectral power, the power between the 0.0 and 0.40 Hz were measured. Measurement of VLF, LF and HF power components were presented in absolute values of power (ms 2 ). Statistical analyses The statistical package SPSS (Statistical Package for the Social Sciences, Version 11.5, SSPS Inc, Chicago, Ill, USA) was used for statistical analysis. Continuous variables were expressed as means ± standard deviation. All continuous variables were checked with the Kolmogorov-Smirnov normality test to show their distributions. Continuous variables with normal distributions were compared using the unpaired Student t test. Continuous variables with abnormal distributions were compared using the Mann-Whitney U test. For categorical variables, the chi-square test was used. Values for P<0.05 were considered statistically significant. Results During the admission, the mean disability score was 3.4 ± 0.9 (range, 2-5). None had fluctuating blood pressure. During the 24-h electrocardiogram recording, the mean heart rate was 97.6 ± 14.5 beat/min. There was no abnormal sweating nor orthostatic dizziness noted in mobile patients during the course of their illness. One patient had difficulty in urination (4 th patient), one had urinary incontinence (8 th patient) and one had constipation (12 th patient) [Table - 1] and [Table - 2]. In two of the patients, SSR couldn't be elicited. In the rest of the patients, amplitude of SSR was found to be decreased when compared with the control subjects (P=0.004). The latency of SSR was relatively longer, but the difference between the patients and control group was not significant (P=0.064). In the time domain analysis of the 24-h electrocardiogram consisting of SDNN, SDANN, SDNNindex and in the frequency domain analysis consisting of HF, LF, VLF and total power, the values were found to be decreased in patients when compared with control subjects (P<0.05) [Table - 1] and [Table - 2]. When the mean values with standard deviations of controls were compared with the patients' values one by one, two or more HRV parameters were abnormal in all patients. The pregnant patient with AMAN had increased HRV parameters, and the remaining 13 patients had decreased values. Except for the third patient, SSR was abnormal. SSR was normal only in one patient (the 3 rd patient). SSR couldn't be elicited in the 12 th and 13 th patients, and 11 patients had increased latency or decreased amplitude [Table - 2]. SSR and HRV were both abnormal in 13 patients, and the disability score ranged from 2 to 5. The hospitalization period was 16.7±15.8 days (4-64). The hospitalization period of the pregnant woman who had AMAN was 64 days. We can not say that there was a correlation between the disability score and the hospitalization periods of the patients, because some patients showed improvement more rapidly in spite of the high disability score. The last disability score values evaluated after the last control (10.3±11.6 weeks, 4-48 weeks) ranged from 0 to 3 (1.1±1.1) [Table - 3]. The 12 th patient was a 29-year-old pregnant woman with a gestational age of eight months. She had AMAN, and her disability score was 5. Her SSR couldn't be elicited, and two parameters of HRV were found to be increased. On the first day of hospitalization, she required mechanical ventilation which lasted 30 days. For maternal stabilization, her baby was delivered by caesarean section on the same day. She was treated with plasmapheresis five times followed by 0,4 g/kg/day intravenous immunoglobulin for five days. After two months of hospitalization, she was discharged with a disability score of 4 for the purpose of applying to a rehabilitation center. After one year, her disability score was 3, which we learned by telephone. The ninth patient, the other pregnant woman, was 17 years old with a gestational age of seven months. She had AIDP, and her disability score was 4. She was treated with plasmapheresis five times. On the 10th day of hospitalization, her score was 2. The pregnancy continued uneventfully, and two months later she delivered two healthy babies, and her motor strength was normal. The first patient, a 52-year-old man, applied to the clinic in the second month of the disease while he was in the convalescence state. His disability score was 3, and any specific therapy was not given because of the given history associated with prominent improvement. Discussion Cardiovascular autonomic neuropathy is a common and potentially life-threatening complication in GBS, however, quantitative tests to assess such patients have rarely been used. This has been attributed to the fact that severely affected patients are unable to perform standardized tests of autonomic function in an appropriate fashion. [11] SSR and HRV analysis are non-invasive and easily applicable, requiring no active motor tasks, and are therefore feasible, even in severely affected patients. [3],[8],[9] SSR is commonly used for the assessment of autonomic nervous system function because of its easy application and reliable results. The wave itself reflects temporary change in electrical potential generated in the deep layers of the skin, the consequences of internal or external stimuli (including deep inspiration, coughing, painful stimuli, or electrical impulses applied to peripheral nerves). The wave is thought to originate from synchronized activation of sweat glands in response to a volley of discharges by efferent sympathetic nerve fibers. The final efferent pathway of the SSR begins within the thoracolumbar cord and is mediated by the unmyelinated postganglionic sympathetic fibers. Experimental studies have demonstrated that the probable generators of SSR are the posterior hypothalamus or the mesencephalic reticular formation. [5],[12] We found only one study associated with SSR in GBS in the English literature in Pubmed and in that study, the authors reported absent SSR in nine of 24 patients with GBS. [6] We couldn't get SSR in two patients and the rest of the patients had lower amplitude when compared with the control group. These results indicate an involvement of sympathetic activity in our patients. Normal HRV depends on the balance between the sympathetic and parasympathetic systems. A high variability in heart rate is a sign of good adaptability, implying a well-functioning autonomic control mechanism. The loss of HRV and sympathovagal imbalance is known to predispose to arrhythmogenesis in both clinical and experimental conditions. HRV analysis is a practical, reproducible and noninvasive method to assess sympathovagal modulation of cardiovascular function in normal healthy individuals and patients with various cardiovascular and noncardiovascular disorders. [13] There are two approaches to measure HRV: time domain and frequency domain analysis. In time domain analysis, SDNN represents a general measurement of autonomic nervous system balance, whereas pNN50 and RMSSD predominantly reflects parasympathetic activity. In frequency domain analysis, HF is modulated predominantly by the parasympathetic nervous system, whereas the LF is under the influence of both the parasympathetic and sympathetic systems. The LF/HF ratio can be considered to be a marker of the sympathovagal balance. [13],[14],[15] There have been three studies on power spectrum analysis of HRV in patients with GBS by Flachenecker et al., in the English literature. [8],[9],[16] In one of these studies, the electrocardiogram was recorded continuously for 5 min. [16] In two of them, 24-h recordings were elicited. [8],[9] Their results suggested that 24-h heart rate power spectrum may yield more sensitive and specific markers to assess the risk of impending and potentially life-threatening autonomic dysfunction and therefore arrhythmias. We studied the time and frequency domain analysis of HRV gathered from a 24-h electrocardiogram recording in patients with GBS who didn't have any pre-existing diseases to rule out their possible effects on the autonomic system. The recording was obtained immediately after admission without the patients receiving concomitant medication. Their results were compared with the control group. In the time domain analysis, the decrease in SDNN, SDANN, and SDNN-index reflected an involvement of a general autonomic nervous system balance. In the frequency domain analysis, the decrease in HF, LF, VLF and total power reflected an involvement of both the parasympathetic and sympathetic systems. When the values of controls were compared with the patients' values one by one, the pregnant patient with AMAN had increased HRV parameters, and the remaining 13 patients had decreased values. This difference suggests a failure in the autonomic nervous system of AIDP patients, and overactivity in the autonomic nervous system of the AMAN patient. In a study by Asahina et al., the patterns of autonomic dysfunction for the two subtypes of GBS, AMAN and AIDP, were also found to be different. They reported that the AIDP patients showed hyperactivities of the cardio-sympathetic system, and the AMAN patients had normal cardio-vascular autonomic function. This is a unique report on the differences of autonomic manifestations between AIDP and AMAN. [17] The limitations-of this study include the number of the patients and pharmacological heterogeneity of the GBS group. In summary, the results of both SSR, and the time and frequency domain indexes of a 24-h electrocardiogram recording were compatible with an autonomic involvement including both parasympathetic and sympathetic components in our GBS patients. Our results suggest that SSR and HRV parameters may be used for early detection of any autonomic dysfunction in patients with GBS. Cardiovascular response may be different in AMAN and AIDP patients, and this difference may play a role in the underlying pathogenesis of the severity of the clinical outcome. More conclusive results may be gained with larger study groups comprised of different subtypes of GBS. References
Copyright 2010 - Neurology India The following images related to this document are available:Photo images[ni10103t3.jpg] [ni10103t2.jpg] [ni10103t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}