 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
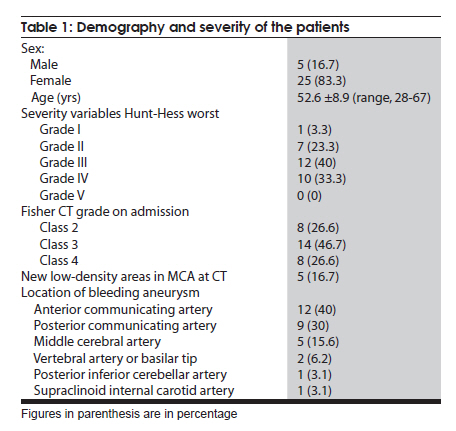
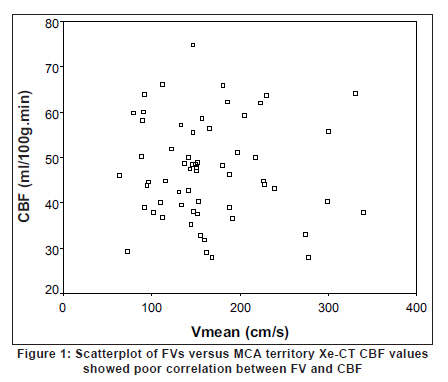
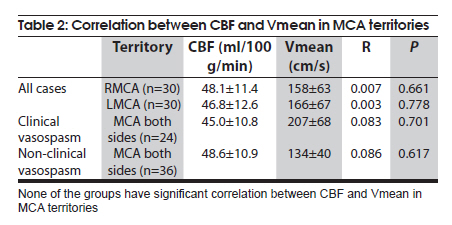
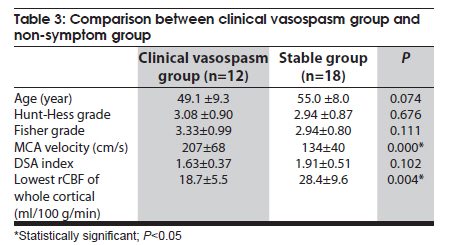
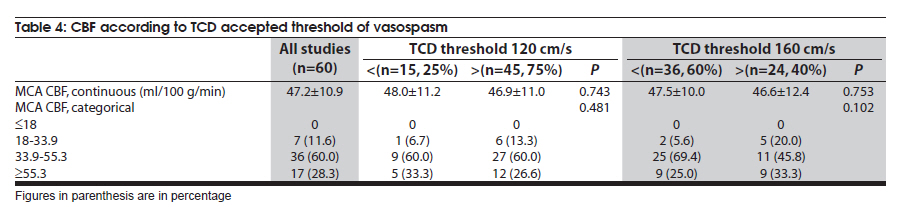
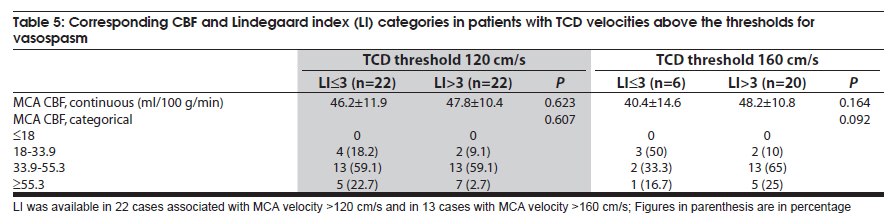
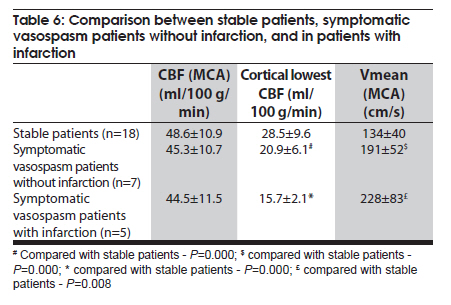
Neurology India, Vol. 58, No. 3, May-June, 2010, pp. 407-411 Original Article Xe-CT and transcranial doppler in symptomatic vasospasm subarachnoid hemorrhage patients under euvolemic treatment without sedation Yueqiao Xu, Yabing Wang, Yuhai Bao, Hongqi Zhang, Feng Ling Department of Neurosurgery, Capital Medical University, Xuanwu Hospital, 45 Changchun Street, Beijing - 100 053, China Date of Acceptance: 20-Apr-2010 Code Number: ni10105 PMID: 20644269 Abstract Background : Delayed cerebral ischemia from cerebral arterial vasospasm following aneurysmal subarachnoid hemorrhage (aSAH) is associated with significant morbidity and mortality. Early recognition of the cerebral arterial vasospasm and institution of appropriate treatment can reduce the consequences. Keywords: Cerebral vasospasm, subarachnoid hemorrhage, transcranial doppler sonography, xenon-enhanced computed tomography Introduction Delayed cerebral ischemia from cerebral arterial vasospasm after aneurysmal subarachnoid hemorrhage (aSAH) is associated with significant morbidity and mortality. Angiographic vasospasm occurs in about 75% of patients following aSAH [1] and symptomatic vasospasm occurs in 26.5-46% of patients. [2],[3] Transcranial Doppler (TCD) ultrasonography is the noninvasive investation modality commonly used to detect arterial vasospasm. However, flow velocities estimated by TCD may not help in assessing the degree of cerebral vasospasm and the clinical development of delayed ischemic deficit. [4],[5],[6] Stable xenon-enhanced computed tomography (Xe-CT) provides rapid access to high-resolution quantitative local cerebral blood flow (CBF) information coupled with CT anatomy [7] and has been used to assess symptomatic vasospasm. [8],[9] We investigated the association of TCD and Xe-CT (not sedated) in patients with symptomatic vasospasm following aSAH, on euvolemic treatment without sedation. Materials and Methods The study has been approved by the local Institutional Review Board, Xuanwu Hospital and procedures followed were in accordance with the ethical standards of the local committee on human experiment and with the Helsinki Declaration of 1975, as revised in 2000. Study subjects were recruited from consecutive patients admitted to the Intensive Care Unit of the Neurosurgery Department. Inclusion criteria included: arrival at the hospital within 72 h of onset of aSAH proven by digital subtraction angiography (DSA), successful clipping or emblazing within 24 h of admission; both TCD and Xe-CT examinations should have been done on the same day within four to nine days of onset of aSAH with clinically stable condition, stable spontaneous respirations without support, and sufficient data for analysis. General patient management involved: control of intracranial pressure (ICP), sedation when necessary, and euvolemic treatment. Shortly after successful embolization or surgery, an intraventricular catheter was placed to measure ICP and to treat hydrocephalus in patien with Hunt-Hess Grade 4 or more and in patients with Hunt-Hess Grade 2-3, ICP was controlled by intermittent cerebrospinal fluid (CSF) lumbar drainage. Bone flap was not replaced in patients with intracerebral hematoma and brain bulg. The target for ICP was below 20 mmHg and for cerebral perfusion pressure (CPP) was about 70 mmHg. Central venous pressure (CVP) was kept at 5-8 with 0.9% saline, colloid, and albumin. Fluid input was maintained at approximately 4 L and adjusted according to the output and body weight. Hypertension was only treated if systolic blood pressure (SBP) >180 mmHg, diastolic blood pressure (DBP) >100 mmHg, or mean artery pressure (MAP) >120 mmHg. In patients with symptomatic vasospasm, SBP was allowed up to 200 mmHg, DBP up to 120 mmHg, and MAP up to 140 mmHg. Propofol or midazalom was used for sedation when required and was stopped at least 4 h before Xe-CT and TCD examination. Patients were put on nimodipine 60 mg q6 for vasospasm prophylaxis and phenytoin for seizure prophylaxis. Fever was controlled by acetaminophen and cooling blankets, and serum Na + was monitored and adjusted to 135-145 mmol/L. Confounding variables that affect regional CBF (rCBF) and blood velocity like hematocrit, PCO 2 , and blood pressure, were similar at the time TCD and Xe-CT studies. Symptomatic vasospasm was a diagnosis of exclusion and was primarily based on unexplained global or focal neurological deterioration onset without hydrocephalus, hemorrhage, surgical complications, metabolic abnormalities, or infection. [2] Daily detailed neurological examinations were performed by the same neurosurgery staff members. Neurological worsening was defined as a decline of at least two points in the modified Glasgow Coma Scale or an increase of at least two points in the abbreviated National Institutes of Health Stroke Scale. [10],[11],[12] When patients were not evaluable neurologically, symptomatic vasospasm was defined as clinical signs of vasospasm (e.g., new neurological deficit) with vasospasm on DSA or TCD, or when a new hypodensity was observed on a post-procedure CT scan. TCD criteria for vasospasm were a Lindegaard ratio >3, a mean middle or anterior cerebral artery flow velocity >200 cm/s, or an increase >50 cm/s/24 h. [13] Other causes of neurological worsening were excluded. Baseline TCD studies were performed within the first two days of admission and again during the high-risk vasospasm period (four to nine days of aSAH). All TCD values were measured with a standard TCD machine (Companion 3 8080; Viasys Healthcare, Los Angeles, CA, USA) using a 2 MHz, pulsed, range-gated transducer. [14] The Lindegaard index was calculated as a reference. [13] The TCD studies were performed within 2 h of Xe-CT studies by an experienced examiner who was unaware of the Xe-CT scan results. CBF studies were performed within four to nine days of aSAH using a CT scanner equipped for Xe-CT CBF imaging (Xe/TC system-2; DDP Inc., Houston, TX, USA). In our hospital Xe-CT facility is available only on every Tuesday. The wash-in protocol was performed as previously described. [7] The scan was performed using four contiguous 10 mm axial sections separated by 20 mm intervals. Regions of interest (ROIs) were centered on the cortex and were divided into six ROIs according to big artery territories on each level by computer software. The CBF calculation involved the two central levels on the middle cerebral artery territory. The mix median cortical CBF was performed by dedicated software (Xe-CT system version 1.0w; Diversified Diagnostic Products, Inc, Houston, TX, USA). The lowest cortical CBF was selected from the 20 ROIs that were automatically divided by computer software. DSA was performed by the interventional neuroradiology team. Neuroradiologists who were unaware of other diagnostic results and clinical information measured the arterial calibers with the ruler tool of the DSA equipment. Magnification corrections were made using internal carotid artery (ICA) diameters in the extradural area as references. Angiographic vasospasm was diagnosed by the criteria as previously described. [15] Two sets of data were obtained for each coupled study; i.e., the CBF and TCD data independently measured on either side. Consequently two sets (one for each anatomical side) of paired (CBF and TCD) data from the same patient were analyzed. The correlation was independently applied to each data set with respect to the right and the left anatomical sides. However, due to the small number of cases, the correlation between CBF and Vmean of MCA in subgroups of patients was calculated based on data from both anatomical sides. Data concerning CBF associated with the critical or subcritical levels of Vmean were compared by parametric or nonparametric methods, or by χ2 test. A P value below 0.05 was considered statistically significant. Analysis was performed using the SPSS 11.0 software (SPSS Inc. Chicago, IL, USA). Results Of the 98 consecutive patients with aSAH admitted during the study period, paired Xe-CT and TCD studies were performed in 39 patients. Nine patients had head movements during Xe-CT study and a poor quality scan. Thus, only 30 patients were available for the analysis. Patient characteristics are shown in [Table - 1]. Most patients had moderate or severe aSAH (73%, Hunt-Hess Grade 3-4), and were at high risk for vasospasm on CT findings at admission (73% patients with Fisher Grade 3 or 4). Of the 30 patients, 12 (40%) patients developed clinical vasospasm, typically between day 4 - 14 of SAH, diagnosis confirmed by DSA. Clipping was done in 18 patients and 12 patients had embolization, mean time of 36±19 h (range, 12-75 h). Six (20%) patients underwent external decompression, 12 patients were treated by ventricle drainage, and 17 patients were treated with lumbar drainage. Of the 30 aneurysms, 18 aneurysms were located in the anterior circulation. There was no correlation between CBF and mean MCA territory velocity (Vmean) [Figure - 1] in all the patients [Table - 2]. The distributions of CBF with respect to the two different TCD thresholds are shown in [Table - 3]. There were no differences in CBF categories. The distributions also revealed that the majority of the CBF of MCA were hyperemic (88%, >33.9 ml/100 g/min). The Lindegaard index was available in 22 paired TCD and Xe-CT studies, mean value 3.17±0.66. The relationship between the TCD thresholds, Lindegaard index threshold, and CBF is shown in [Table - 4]. There was a significant decrease of the lowest cortical CBF and an increase in the MCA blood flow velocity in the clinically symptomatic vasospasm group compared to the non-symptom group [Table - 5]. Five cases developed infarction in the follow-up CT scans. In these five cases, the lowest CBF was 15.7±2.2 ml/100 g/min, lower than in patients without symptoms (28.5±9.6, P=0.000); the lowest CBF also trended lower than in patients with symptoms but without infarctions (N.S.; [Table - 6]). The Vmean of MCA was lower in the stable group than the symptomatic vasospasm group (P<0.05). Discussion Mean blood flow velocity of the MCA is used widely for the diagnosis of vasospasm fallowing aSAH. In the present study there was poor correlation between the mean flow velocity and measured cortical mixed CBF in the MCA territory, both in patients with and without symptomatic vasospasm, thus suggesting that the MCA velocity as measured by TCD may not predict rCBF of the MCA. Lindegaard index also could not predict rCBF of the MCA territory. The mean CBF of the MCA territories were not significantly decreased even in patients with symptomatic vasospasm. The mean velocity of the MCA in patients with clinical vasospasm was higher than in stable patients, while the lowest rCBF values were lower in symptomatic vasospasm patients than in the stable patients. In the present study the elevated Vmean values were not specifically associated with an ischemic rCBF in the MCA territory. These findings are similar to a study in poor-grade SAH patients undergoing aggressive ICP management. [16] In this study the mean CBF was much lower than in our study (35.1 vs. 47.2 ml/100 g/min). The authors suggested that the velocity/CBF mismatch might have been resulted from sedation, and that burst suppression might have reduced oxygen metabolism and thus reduced CBF. But increase in microvascular resistance; circulation support may weaken the relationship between clinical vasospasm, TCD vasospasm, and angiographic vasospasm. In our study, hypertensive, hypervolemic, and hyperdilational (3H) treatments was instituted in patients with clinical vasospasm and 3H therapy might have weakened the correlation between MCA velocity and CBF. CBF definitions based on Xe-CT study in aSAH include: irreversible ischemia (CBF <10 ml/100 g/min), ischemia penumbra (CBF 10-20 ml/100 g/min), oligemia (CBF 20-34 ml/100 g/min), relative hyperemia (CBF 34-55 ml/100 g/min), and absolute hyperemia (CBF >55 ml/100 g/min). [17] In majority of our patients, MCA CBF was relatively in hyperemic range. In the earlier studies in patients with clinically symptomatic or TCD vasospasm treated with 3H therapy, wide range of cerebral percussion disturbances have been described. [18],[19] However, both these studies [18],[19] had not addressed the issues of sedation or optimal control of ICP. In the present study, the mean velocity of MCA in patients with clinical vasospasm was significantly higher than in stable patients, suggesting that TCD blood flow velocity measurement may be a good invasive screening method to predict clinical vasospasm. However, the thresholds should be adjusted in patients who undergo 3H treatment or euvolemic support. In our patients the Vmean increased in patients with symptomatic vasospasm. Compared to the rCBF of the MCA territory, the lowest cortical rCBF is more useful for the diagnosis of symptomatic vasospasm. The CBF of the MCA territory may be more useful when adjusted for 3H, and the CBF of the distal small vessel territory still reflects the insufficient blood supply during vasospasm. Xe-CT measurements can be useful for the management patients with aSAH as these measurements reflect the potential perfusion alterations induced by vasospasm. [20],[21],[22] Results from our study suggest that TCD data should be more carefully interpreted in patients on 3H treatment. The CBF thresholds in Xe-CT studies may also require adjustment according to the patient's clinical condition. [23] A limitation of our study is small number of patients. Potential limitations of the TCD technique are related to the experience of the operator. Nevertheless, with experienced operators the inter-observer reproducibility is high, especially in the middle cerebral artery. [24] As patients were not sedated during Xe-CT examination and nine patients were excluded because of poor quality of scans as result of head movement. This might have lead to some patient selection bias. Acknowledgments The authors gratefully acknowledge experimental participation of the technicians at the TCD Lab as follows: Yang Hua, Yumei Liu and Chun Duan. References
Copyright 2010 - Neurology India The following images related to this document are available:Photo images[ni10105t5.jpg] [ni10105t4.jpg] [ni10105t2.jpg] [ni10105t3.jpg] [ni10105f1.jpg] [ni10105t6.jpg] [ni10105t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}