 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
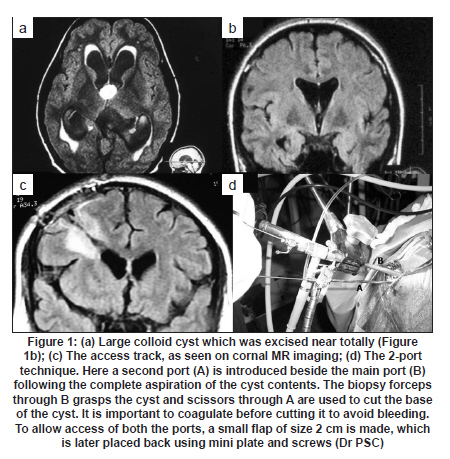
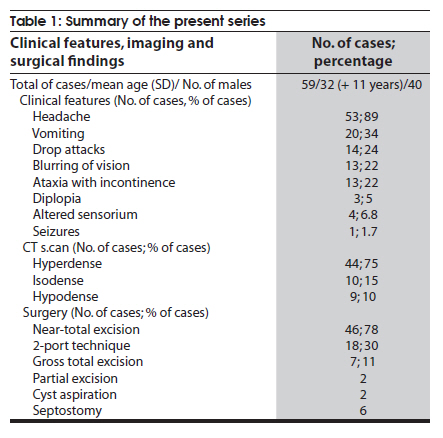
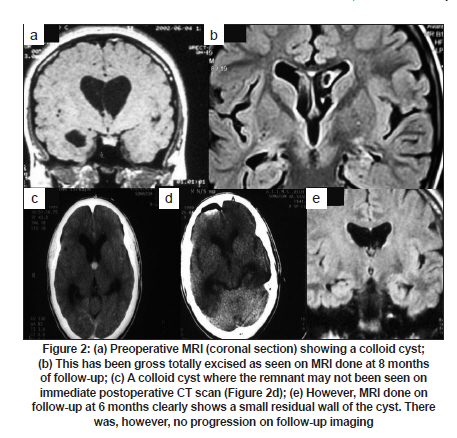
Neurology India, Vol. 58, No. 3, May-June, 2010, pp. 412-417 Original Article Endoscopic management of third ventricular colloid cysts: Eight years' institutional experience and description of a new technique Shashwat Mishra, P Sarat Chandra, Ashish Suri, K Rajender, Bhawani S Sharma, AK Mahapatra Department of Neurosurgery, All India Institute of Medical Sciences, New Delhi - 110 029, India Date of Acceptance: 01-Feb-2010 Code Number: ni10106 PMID: 20644270 Abstract Background : The operative approaches for colloid cyst excision are varied with open microsurgical excision still being considered as the "gold standard". Endoscopic removal of these cysts is gaining in popularity. Keywords: Colloid cyst, endoscopy, near-total excision, third ventricle Introduction Colloid cyst of the third ventricle is an uncommon lesion and the reported incidence is 3.2 per 100,000 population. [1] The natural history is varied and most of the patients have an insidious course. However, some of the patients present with sudden neurological deterioration: drop attacks; life-threatening acute hydrocephalus; and sudden death. [1],[2],[3] Even though the treatment approach for asymptomatic incidentally detected colloid cysts is debatable, most neurosurgeons advise intervention to avoid catastrophic neurological deterioration. However, long-term follow-up study of 68 subjects with asymptomatic colloid cysts suggests that only a few (8%) subjects go on to develop symptoms at 10 years. [4] The surgical approach for symptomatic colloid cysts is varied. The operative procedures usually consist of open microsurgical excision techniques. [1],[2],[5],[6],[7] Less often stereotactic aspiration or stereotactic-guided surgery have been described. [8],[9],[10],[11] Endoscopic approach for excision of colloid cysts is relatively recent and offers the advantage of excellent visualization and minimally invasive corridor through the naturally dilated ventricular system. A more controlled resection of the cyst is possible through this approach avoiding damage to critical structures in the anterior third ventricle. We share our experience with the endoscopic approach to colloid cyst resection and also describe a new two-port technique for achieving near-total excision. Materials and Methods During the study period, January 2001 till May 2009, 59 patients with colloid cyst were operated by endoscopic approach. Preoperatively all the patients had contrast magnetic resonance imaging (MRI). All the patients had hydrocephalus. Two patients underwent endoscopic resection for recurrent cysts, one patient had open surgery and the other endoscopic resection at the other facility. Surgical planning The approach was from the right lateral ventricle except in patients with asymmetric dilatation of the ventricles in which case the access was attempted from the side of maximally dilated lateral ventricle. Mid-sagittal MRI section was utilized in planning the burr hole location and the endoscopic trajectory for optimal visualization of the colloid cyst. Sometimes the cyst was completely intra-third ventricle and was posterior in location with respect to its usual location at the foramen of Monro. In such cases the burr hole was placed more anterior and the actual location deduced by joining a line from the center of the cyst to the foramen of Munro and extrapolated to the skull surface. The actual anatomical location was always planned after careful study of both saggital and coronal MR images which helped to define the relationship of the cyst with respect to the ventricular structures. The coronal image on MRI was particularly useful to decide the side of approach. Surgical technique All the patients underwent the procedure under general anesthesia. Patients were positioned supine with the head resting on a doughnut pillow in the neutral position. The burr hole position, though roughly described as precoronal frontal burr-hole, was adjusted to the location of the colloid cyst with respect to the structures around the foramen of Munro. Generally, the burr hole corresponded to a point 4 to 5 cm away from midline and 4 cm anterior to the coronal suture. We used a freehand cannulation of the ventricles with the endoscope sheath and the obturator. In most of the patients, an obturator telescope was used which enabled visualization of the path of entry. We only used rigid endoscopes because of their superior optics and safer maneuverability inside the ventricular system. Flexible scopes were used whenever inspection within the lateral ventricles was required, e.g. to look at the end of the surgical procedure. After ventricular puncture, the obturator was withdrawn and the endoscope introduced to visualize the foramen of Munro, the septum pellucidum, thalamostriate vein and the choroid plexus. In most of the cases the colloid cyst was seen bulging through the foramen of Monro into the ipsilateral lateral ventricle. The endoscopic coagulator was then introduced. The cyst wall was then coagulated carefully allowing the vascular fibrous outer layer to shrink towards the probe, avoiding contact of the probe with normal ventricular structures at all times. The cyst wall was cut open by endoscopic scissors. Once this was done, a Fogarty balloon was inserted through the cyst wall and inflated to enlarge the opening. Thereafter, the cyst contents were aspirated. We developed the following technique to perform cyst content aspiration. The cystic contents are suctioned through a long narrow metallic suction tube which is connected via a three-way luer lock stopcock to the vacuum generator through one port and to a 50-cc syringe via another port. The thick viscous cystic contents are aspirated under controlled suction using the 50-cc syringe while using continuous irrigation with Ringer's Lactate [Figure - 1]. This ensures that the irrigating fluid mixes well with the cyst contents and makes it easier to suck the thick contents. This is the most important step of the procedure and must be done with adequate care. It also becomes necessary in most of the cases to introduce the endoscope into the cyst cavity to make sure that all the contents have been aspirated. Once the contents are aspirated, only the translucent wall is left behind. Following this a biopsy of the wall is required. This is performed by first coagulating the wall and then cutting it using scissors. This technique requires patience on the part of the surgeon. Both the coagulation and cutting with scissors have to be alternated; once the pedicle becomes very thin, the last part may be gently pulled with a biopsy forceps. The residual portion of the cyst attached to the neurovascular structures is coagulated till it shrinks until a small nubbin is left behind. One has to be aware that coagulating smaller cysts can result in cyst shrinking significantly towards the choroid plexus, and this can make cutting and biopsy of the cyst wall difficult. Two-port technique: One of the authors (PSC) has used a novel two-port technique in 18 patients to achieve a gross total excision, particularly in large cysts. A small circular bone flap of size 2 cm is created using B1 Midas Rex pneumatic drill instead of a burr hole. Following the completion of the procedure, the flap is placed back and held in place with mini plate and screws. The rest of the procedure is the same as described above. Once the cyst is completely aspirated, a second port, 3-mm-thick metallic sheath, is introduced alongside of the main port. The cyst is grasped using biopsy forceps from the main port and is cut using scissors from the side port [Figure - 1]. Using this technique a gross total excision is achieved. Minor bleeding during the procedure was generally handled with Ringer fluid irrigation. One of the useful techniques to handle moderate bleeds was to use the metallic suction device at the bleeding point under continuous irrigation with Ringer's lactate through the main port. This avoids the dissipation of the blood into the ventricular cavity thus preventing clouding of the visibility. In order to avoid undesirable hypothalamic stimulation, isothermal irrigation fluids are used. In case of significant intraventricular bleed, a ventricular drain was left in situ at the end of the procedure. The drain was removed after 12-24 h when the cerebrospinal fluid (CSF) became clear. Postoperative management Postoperatively, patients received antibiotics as per the institute protocol. A plain computerized tomography (CT) scan was performed the same day evening to rule out any bleed. If a ventricular drain was placed, it was clamped first and then removed after 12-24 h when the CSF became clear. Follow-up The patients were regularly followed up clinically and radiologically. First follow-up MRI scans were obtained six months post procedure in asymptomatic patients or earlier in patients with recurrence of symptoms. Imaging was repeated at three to five years in asymptomatic patients. Results Of 59 patients, there were 40 males; mean age at presentation was 32 years (±11 years). There were two patients with recurrent cysts and both the lesions recurred four years after the first surgery. The initial procedures on these cysts were performed at other facilities. Most of the patients presented with a non-localizing headache (53; 89%). Other symptoms included: vomiting (20; 34%); drop attacks (14; 24%); blurred vision (13; 22%); ataxia with incontinence (13; 22%); diplopia (3; 5%); altered sensorium (4; 6.8%); and seizure (1; 1.7%) [Table - 1]. Interestingly, 22% of our patients presented with symptoms suggestive of hydrocephalus i.e. urinary incontinence and gait ataxia without headache. In them the mean age at presentation was 44 years. Four patients presented to the emergency in an unconsciousness state and required an emergent external ventricular drain. Non-contrast computerized tomography (CT) head showed the lesion as hyperdense in 44 (75%), isodense in ten (15%) and hypodense in nine (10%) patients. Hydrocephalus was present in all the patients and asymmetric enlargement of ventricles in five patients [Table - 1]. The procedures included gross total excision (total excision except for a small nubbin of cyst wall left along the neurovascular structures) in 46 patients (78%) [Figure - 2]a and b. Of these patients, 18 patients underwent a two-port technique [Figure - 1]. Near total excision (a remnant of cyst wall left behind) was performed in seven (11%) patients [Figure - 2]c-e. Partial excision in five and cyst aspiration only in one patients. Patients who had partial excision and cyst aspiration were the earliest patients when the procedure was first started. Both the patients are being followed up closely for the last six years and have not developed any recurrence. Calcified cyst wall was encountered in one patient with dense adherence to the fornix allowing partial excision only. During attempted cyst wall excision in another case, brisk bleeding was encountered and further procedure had to be deferred and only partial excision of cyst wall could be accomplished [Table - 1]. The mean operating time for procedure was 128 min (SD + 38 min). Septostomy to gain biventricular access was performed in six patients. Bleeding from the colloid cyst bed was the most frequently encountered intra-operative event. It occurred mostly towards the end of the procedure when the cyst wall was being separated from the choroid plexus and the forniceal columns. In most of the patients, it was controlled with prolonged irrigation with Ringer's lactate. However, in 14 patients, intraventricular bleed was significant and it was deemed necessary to leave an external ventricular drain. Intraventricular drains were used even in patients with minor persistent ooze or cloudy CSF because of the dissipation of the colloid material in case of large cysts. Ectopic rhythms were seen in one patient at the time of manipulation of the colloid cyst wall. Following surgery, headache improved in 51 (96%) patients in whom headache was the initial presenting symptom. Vomiting, drop attacks, blurring of vision improved in all. Diplopia improved in two patients. One patients continued to have diplopia on extremes of gaze. There was one death related to meningitis. This was in a patient who presented in altered sensorium with acute hydrocephalus and had to undergo an external ventricular drainage followed by definitive surgery. Two patients required VP shunt after cyst excision for the symptomatic hydrocephalus. Other complications included burr hole site epidural hematoma (1), cerebellar hematoma (1), CSF leak from burr hole site (1) and acute hyponatremia (1). All these complications were managed medically and recovered. The average postoperative hospital stay in uncomplicated cases was four days. Follow-up The mean follow-up was 13+ 19.2 months (range; 3 weeks- 99 months). Follow-up imaging was available in 41 patients and revealed a small residual cyst in five patients. None of the patients with residual cysts required re-operation. They are under regular follow-up and were asymptomatic till the last visit. Discussion Colloid cysts occur most commonly in the fourth through seventh decade [2],[9],[13],[15] Similar were the observations in our series. The symptom profile in our patients was similar to the other reports. [1],[2],[5],[10],[11],[12],[13],[14],[15],[16],[17],[18],[19],[20] About 22% of patients in this series had triad of memory loss, gait abnormality and incontinence, symptom complex of normal pressure hydrocephalus. The mean age of these patients at presentation was 44 years. The optimal surgical management of colloid cysts continues to be a matter of debate. Colloid cysts are benign lesions with low risk of recurrence after radical resection. Open microsurgical excision was traditionally considered the "gold standard" treatment. However, operative approaches are not without risks. Of the 38 patients who underwent transcortical-transventricular resection of the colloid cyst, 30% of patients had postoperative complications. [2] Transcallosal approach avoids the potential risks of a cortical incision, but still is associated with occasionally serious morbidity. The reported complications of this approach include cortical venous infarct, forniceal damage, injury to the deep venous system, subdural hematoma, disconnection syndromes, ventriculitis and meningitis. [1],[6],[8],[13] The quest for less invasive approaches for deal these lesions, led to the introduction of aspiration techniques for decompression of the cyst. Free-hand aspiration of colloid cysts was attempted in 1975 by Gutierrez-Lara, et al.[20] To increase the accuracy of the procedure, stereotactic guidance was employed first by Bosch and co-workers [21] and it gradually gained popularity, because the procedure is associated with negligible morbidity. However, it was soon realized that not all colloid cysts could be suitable for aspiration and high viscosity of the cyst contents seriously limited the evacuation of cyst material. [9],[10],[11] Kondziolka and colleagues [11] had found that only cysts which are hypodense or isodense on plain CT may be amenable to successful aspiration. More than two-thirds of colloid cysts were found to be CT hyperdense in their series, similar were the observations in our series. Moreover, leaving the mucin-secreting wall behind after aspiration increases the possible risk of recurrence. [9] Endoscopic transventricular resection strikes a fine balance between the morbidity of open surgery and the low efficacy of needle aspiration. Powell et al. are credited with the first successful endoscopic aspiration of the colloid cysts. [14] Auer et al.. used a neodymium:yttrium-aluminum-garnet laser to endoscopically coagulate the cyst wall. [15] Lewis and Kohler have compared craniotomy and endoscopic procedures for colloid cyst resection and have found shorter operative times and hospital stay in patients undergoing endoscopic surgery. [5] The efficacy of neuroendoscopic techniques for colloid cyst resection has been well established in several studies. [17],[18],[19],[22],[23],[24] Transcallosal microsurgical resection continues to be benchmark against which all other operative techniques are compared. However, technically, the endoscope may have several advantages over the microscope. Rapid improvement in endoscopic instrumentation is further increasing the versatility of the endoscope. Endoscope offers superior illumination, greater magnification and enhanced visualization of the ventricular anatomy. With angled endoscopes, it is possible to see the roof of the third ventricle and thus the point of attachment of the colloid cyst aiding in radical excision of the cyst. Such a view of third ventricular roof is often not possible even with the direct transcallosal approach unless an interforniceal corridor is used. This procedure is associated with risk of damage to the bilateral fornices. [24],[25],[26] The transcortical, transventricular approach overcomes this disadvantage but then again involves excessive manipulation of the fornix to visualize the roof of the third ventricle. Furthermore, colloid cysts are not tumors but developmental lesions and cure may be achieved even if a small residue is left behind, provided that the wall of the cyst is adequately opened up so as not to allow entrapment and cystic recollection. It is to be acknowledged that there is a definitive learning curve associated with the endoscopic treatment of colloid cysts. In our initial patients, we coagulated the cyst wall and aspirated the cyst contents. Later, this was followed by cutting open the cyst wall and coagulating it from inside. Presently we attempt to perform a gross total excision in all cases. Only in cases where this is not possible, we perform a near-total or a partial excision. Development of a two-port technique allows a radical excision in a majority of cases. However, near-total excision can be achieved even with a single port or with use of conventional endoscopic techniques. [8],[19],[23],[24],[25],[26] Ultimately, it is the comfort of the surgeon to achieve a radical excision rather than the number of ports used that matter. With evolution of our own experience, we found that passing a second port does help to significantly enhance the chances of radical excision. Bergsneider [26] had also reported the use of two ports and the second port was introduced through a supra orbital opening (eyebrow). The technique described by us, to the best of our knowledge, has not been described earlier. Till date there was no recurrence of the lesion during the follow-up. In the initial six patients who underwent aspiration and partial excision, the lesion is of the same size on follow-up imaging. The openion is divided over the superiority of radical resection as compared to coagulation of cyst remnants. [8],[19],[23],[24],[25],[26] Although some neuroendoscopists [25],[26] have advocated complete cyst wall excision to prevent cyst recurrence, we had no patient with small residual remanent who had recurrence. The observation in the other studies are similar to our observation. [19],[23] However, the goal should be to perform a radical excision. Radical resection of the colloid cyst requires a certain degree of technical skill and experience with the endoscope and may take some time. None of our cases required conversion to open craniotomy for excessive bleeding or poor visualization of the colloid cyst, which attests to the safety and excellent applicability of endoscopic technique for resection of colloid cysts. Most of the bleeding can be controlled with Ringer's lactate solution. In case of persistent yet minor ooze, a ventricular drain may be left behind to be removed after 12-24h. Sometimes the cyst may be located much more posteriorly hampering proper visualization of the cyst with the endoscope. [17] Although we did not encounter such a situation, we would prefer to approach such lesions through transcallosal approach. Endoscopically resecting such lesions would involve excessive manipulation of the fornix which can potentially cause short-term memory loss. References
Copyright 2010 - Neurology India The following images related to this document are available:Photo images[ni10106f2.jpg] [ni10106t1.jpg] [ni10106f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}