 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
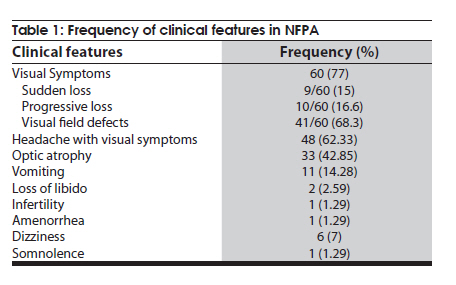
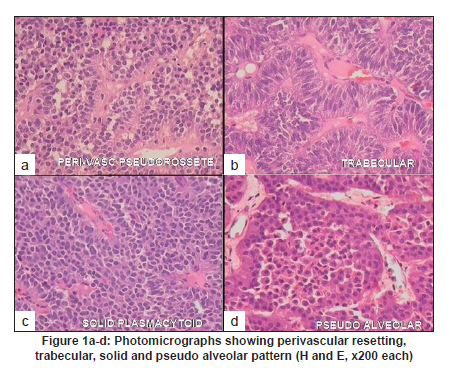
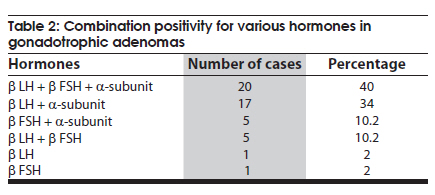
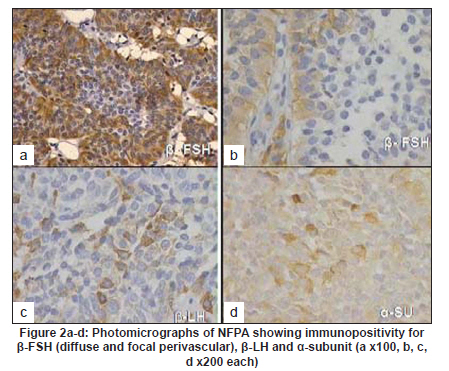
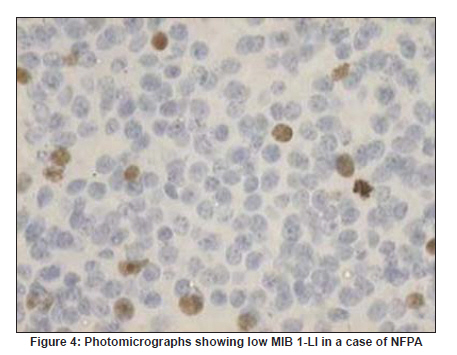
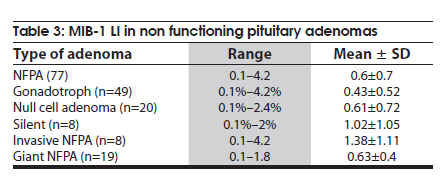
Neurology India, Vol. 58, No. 3, May-June, 2010, pp. 418-423 Original Article A clinicopathological and immunohistochemical study of clinically non-functioning pituitary adenomas: A single institutional experience Arvind Rishi1, Mehar C Sharma1, Chitra Sarkar1, Deepali Jain1, Manmohan Singh2, Ashok Kumar Mahapatra2, Veer Singh Mehta2, Tapos Kumar Das3 1 Department of Pathology, All India Institute of Medical Sciences, New Delhi, India Date of Acceptance: 01-Feb-2010 Code Number: ni10107 PMID: 20644271 Abstract Background : Non-functioning pituitary adenomas (NFPA) are characterized by the lack of clinical syndrome as compared to functioning adenomas (FA) but not all functioning adenomas have clinical effects. Their exact incidence varies in different series. Keywords: Immunohistochemistry, neoplasia, non-functional adenomas, pituitary adenoma, pituitary gland, sellar tumors Introduction Pituitary adenomas are the most common tumors of the pituitary gland and comprise 10-25% of all intracranial tumors. [1] The incidence varies from 20-27% in the autopsy series. [2] Their remarkable variations in the biological behavior have formed the basis for classification into: clinically non-functioning and functioning adenomas. [1],[3] Non-functioning pituitary adenomas (NFPA) comprise 25-30% of pituitary adenomas and are characterized by the lack of hormone-related clinical syndrome as compared to functioning adenomas (FA). [4] Neoplastic transformation may be monoclonal [5],[6],[7],[8] or may affect two different cell populations. [9] NFPA have been shown most commonly to originate from gonadotroph cells and may secrete low amounts of gonadotrophins. Evidence suggests that the majority of NFPA synthesize hormones. Debate exists about whether there is a close relation between null cell adenomas and gonadotroph adenomas or null cell adenomas represent an independent entity. [10] Postoperative radiotherapy significantly reduces the rate of recurrence of NFPA. However, radiotherapy has a significant effect on the biological behavior of NFPA. Thus it is further more important to know about the biological characteristics of these adenomas. [ni11],[12] We undertook this study to analyze the clinical features and hormonal profile of NFPA at the immunohistochemical level in the north Indian population, and to see if any differences exist from the earlier studies. We also evaluated the biological aggressiveness by MIB-1 labeling index (MIB-1 LI) and EGFR expression. All the parameters and the clinical behavior of the tumors were correlated with radiological features of invasiveness or giant size. Materials and Methods All cases of pituitary adenomas diagnosed during one and half years (January 2003 to June 2004) in the Department of Pathology, All India Institute of Medical Sciences, New Delhi were retrieved. The adenomas were classified into NFPA and FA on the basis of preoperative clinical evaluation. Data collected from the case records included: age, sex, clinical features and preoperative size of the adenoma. Based on the radiological and operative findings they were classified into: invasive or giant adenomas. Pituitary adenomas with invasion of cavernous sinus, dura, sphenoid bone and nasopharynx were regarded as invasive adenomas. Pituitary adenomas with size more than 40 mm, or those extending less than 6 mm from the foramen of Monro are classified as 'giant' irrespective of invasiveness. [ni11] Representative blocks of formalin-fixed paraffin-embedded tissues were selected from each case. At least 10 serial 5μ-thick sections were taken on glass slides coated with poly-L-lysine (M/s Sigma, USA). Staining was done with hematoxylin and eosin. Immunohistochemistry (IHC) was done by the streptavidin-biotin immunoperoxidase technique (LSAB) using monoclonal antibodies to human growth hormone (GH, dil 1:500); prolactin (PRL, dil 1:100); adrenocorticotrophin (ACTH, dil 1:600); thyrotrophin (β-TSH, dil 1:200); follicle stimulating hormone (β-FSH, dil 1:200); luteinizing hormone (β-LH, dil 1:200); and α-subunit (dil 1:1000). Immunostaining was also done using antibodies MIB-1 (dil 1:200) and EGFR (dil 1:50). All antibodies except for α-subunit were obtained from M/s Dakopatts, Glostrup, Denmark. Antibody for α subunit was obtained from Serotech. For immunostaining, antigen retrieval was done by microwave boiling of the immersed sections in citrate buffer (10 mMol/L) for 35 min. Antigen retrieval by microwave method was used for of PRL, β-TSH, β-LH, β-FSH, α-subunit and MIB-1 immunostaining. Antigen retrieval for EGFR was done by using protease enzyme for half an hour at 37oC. No antigen retrieval was required for GH and ACTH. Throughout the study appropriate positive and negative controls were used. Negative controls were obtained by omitting the primary antibody. Sections from normal pituitary gland obtained from autopsy specimens were used as the positive controls for GH, PRL, ACTH, β-TSH, β-LH, β-FSH, and α-subunit. Less than 10% immunopositive cells were taken as the cutoff for negative expression of the pituitary hormones. Placenta was taken as positive control for EGFR. Sections from lymph node were used as positive controls for MIB-1 staining. The labeling index (LI) for MIB-1 was calculated as a percentage of labeled nuclei per 1000 cells in the highest proliferating areas. Counting was done at high-power magnification (400x) and an eyepiece pinhole was used to facilitate counting. For all the cases counting was done without knowing the type of adenoma. EGFR expression was taken as either positive or negative based on its membrane expression in more than 10% of the histological section. Results During the study period 151 pituitary adenomas were diagnosed in the Department of Pathology, of which 77 (51%) were NFPA. The mean age at presentation was 46.2 yrs (range 18 to 75 years); 39 (50.6%) patients were between 30-50 years of age, 34 (44%) patients were above 50 years of age and only 4 (5%) patients were below 30 years. There was male predominance with male to female ratio of 2.1:1. The gender distribution was similar patients below 40 years of age; however, males predominance was observed in patients above 40 years of age. This observation indicated that there is increased incidence of occurrence of NFPA with age, which is more apparent in males. The most common presenting symptoms were visual, in 77.9% (60/77), followed by headache (62.3%), vomiting (14.3%), dizziness (7%) hypopituitarism (5.2%) and somnolence (1.3%). Other features such as amenorrhea, loss of libido and infertility were rare in NFPA and observed in one patient each [Table - 1]. Pathologic examination Histopathological examination showed perivascular pseudorosetting as the most prominent pattern (26/77; 33.7%) followed by solid (20/77; 25.9%), trabecular (5/77; 6.5%), papillary (4/77; 5.2%) and alveolar pattern (3/77; 3.2) [Figure - 1]. Oncocytomas, however, constituted only 9/77 (ni11.6%) of NFPA. Hemorrhagic necrosis (apoplexy) was seen in four cases (5.2%). Psammoma bodies and amyloidosis were evident in one case each (1.29%). Rathke's cleft remnants were seen in eight cases (10.3%). Immunostaining showed immunoreactivity for various hormones, either singly or in various combinations, in 83.1% cases (64/77) of NFPA [Table - 2]. On the basis of IHC we classified NFPA into three subtypes: gonadotroph adenomas containing β-subunit of LH and FSH either singly or in combination with α-subunit; null cell adenomas which were negative for all hormones except cases with isolated a-subunit positivity; and silent (non-gonadotroph) adenomas containing PRL, GH or ACTH but not showing any clinical features of hormone secretion. Gonadotroph adenomas were the commonest subtype comprising 64% (49/77) of all NFPA and 32% (49/151) of all pituitary adenomas. This group showed significant hormonal heterogeneity on immunostaining. The intensity of staining varied from diffuse to focal which was especially limited to perivascular areas [Figure - 2]a and b. The most common combination was positivity for all three hormones i.e. b-LH, b-FSH, and a-subunit followed by various other combinations [Figure - 2]c, d and [Figure - 3] [Table - 2]. Null cell adenomas accounted for 26% (20/77) of NFPAs and 13% (20/151) of all pituitary adenomas. Silent (non-gonadotroph) adenomas accounted for 10% (8/77) of NFPAs and 5% of all pituitary adenomas. This group showed plurihormonal immunopositivity in 75% (6/8) and only ACTH in 25% (2/8) but none of them had clinical evidence of hormone hypersecretion. Proliferative index MIB 1-LI was low and ranged from 0.1-4.2% with a mean of 0.6% [Figure - 4], [Table - 3]. Fifty-eight out of 77 cases (88%) showed MIB 1-LI of less than 1%. In invasive and giant NFPA it was on the higher side, however, this difference was not statistically significant. EGFR positivity was noted only in 2 cases of NFPA. Correlation with size and invasion Of 151 pituitary adenomas, 29 (19%) cases were giant adenomas and 12 (8%) cases were invasive adenomas. Of the 12 invasive adenomas, eight (67%) were NFPAs, five (62.5%) null cell type and three gonadotroph adenomas. Nineteen (65%) of the 29 giant adenomas were NFPAs, 13 (68%) null cell type and six gonadotroph adenomas. Of the NFPAs, 19 were giant adenomas and eight (10%) were invasive adenomas. Though, mean MIB 1-LI was high in invasive adenomas compared to giant adenomas, this difference was not statistically significant. Discussion Pituitary adenomas apparently arise from one pituitary cell type or the other and account for 10-25% of all intracranial tumors. [1] Identification of adenomas causing syndrome of hormone hypersecretion is relatively easy on the basis of clinical features, however, pituitary adenomas that do not cause any syndrome of hormone hypersecretion termed "clinically non-functioning pituitary adenomas", are more difficult to diagnose. Any type of pituitary adenoma can be non-functioning and this could be either due to subnormal hormone secretion or due to inability to secrete complete hormone containing both α and β subunits. [13] NFPA are rare in childhood and adolescence [12],[14],[15],[16],[17] and incidence, under the age of 17 years, varies from 2% and 6%. In the study by Mindermann and Wilson, only 6% of patients were under 20 years of age. [18] In our series, there were only two (2.5%) patients below the age of 20 years. NFPA most commonly occurs in the fifth to ninth decades [18],[19],[20] and the age range distribution is quite variable from 16-70 years. [19],[21] In the present study 65% patients were between the ages of 30-60 years. In several series of NFPAs there was male predilection, [22],[23],[24] similar to our series. In the study of NFPAs by Mindermann and Wilson [18] female predilection was noted in patients aged below forty years and male predilection in the older age group. Similar were the findings in our study. In patients with NFPAs, visual symptoms are the most common clinical presentation as seen in this series. [25],[26],[27] Gonadotroph adenomas account for a significant proportion of pituitary adenomas and the reported frequency varies from 3.3% to 24%. [28],[29],[30],[31] In the present series the majority of NFPA showed presence of hormones on immunostaining and gonadotroph adenomas were the commonest subtype accounting for 64% of NFPAs. Adenomas with α-subunit positivity were considered as null cell adenomas in the present study and they accounted for 26% of NFPAs. In the large series by Kovacs et al., [22] null cell adenomas accounted for 16.5% of all pituitary adenomas. The majority of null cell adenomas were negative for all hormones (65%) but 35% were only positive for α-subunit. Expression of α-subunit along with TSH, LH and FSH have been shown in a few adenomas.[32],[33],[34],[35] These observations support the view that there could be only α-subunit production without the concomitant production of β-subunit. Our observations in regard to silent adenomas and NFPAs are similar to the earlier studies. [36],[37] The incidence of silent adenomas in the present series was 10% with male predilection. In an earlier study 4% of clinically silent adenomas were positive for ACTH staining with male gender predilection. [38] Male gender predilection was also observed in another study of 23 clinically silent corticotroph adenomas. [39] Recently, Tateno et al., found no expression of genes related to proopiomelanocortin transcription, synthesis, processing, and secretion in NFPAs in comparison to ACTH-secreting adenoma. [40] Bradley et al., observed aggressive behavior of ACTH-positive NFPAs. [41] They further concluded that if recurrence does occur these tumors tend to follow a more aggressive course and need careful monitoring. Low MIB 1-LI in NFPAs as observed in our study has also been reported in the earlier studies. [42],[43] In most studies there was no correlation between MIB 1-LI and age, sex or duration of symptoms. [43],[44],[45] However, the study by Mastronardi et al.,[42] reported higher MIB 1-LI in patients aged above 65 years. In our study MIB 1-LI was not significantly high in invasive and giant adenomas. Probably it may be related to lesser number of cases in these two groups. Similarly, Yonezawa et al.,[46] also did not find any correlation between MIB 1-LI and invasiveness or recurrence of pituitary adenomas.Abe et al.,[44] could not find any significant correlation between proliferative potential, hormonal status and tumor size. Hentschel et al., have not found any correlation between p53 and MIB 1 immunoreactivity and recurrence of NFPAs. [47] However, Wolfsberger et al.,[48] considered MIB 1 as a gold standard to assess cell proliferation, especially in NFPAs in particular relevance to postoperative management. The present study showed immunopositivity for EGFR in only two cases. The expression of EGF and EGFR is variable in the normal pituitary as well as in pituitary adenomas. [49],[50],[51],[52] Chaidarun et al.,[51] had demonstrated over expression of EGFR in most NFPAs, but absent in the hormone-secreting adenomas. Theodoropoulou et al.,[52] found expression of wild type of EGFR in a high percentage of hormone-secreting adenomas, while no expression of the mutated EGFR could be detected in any of the subtypes including NFPAs. These observations suggest that EGFR expression, needs further characterization in the various subtypes of pituitary adenomas. Our study supports the hypothesis that NFPAs probably have a defect in one or more processes of the hormone biosynthesis and secretion. The present series also proposes immunohistochemistry as an important modality for diagnosing the subtypes of clinically NFPAs, especially gonadotroph adenomas. This will help in selecting such patients for adjunctive medical therapies that are currently under evaluation. References
Copyright 2010 - Neurology India The following images related to this document are available:Photo images[ni10107f4.jpg] [ni10107f3.jpg] [ni10107f1.jpg] [ni10107t2.jpg] [ni10107t1.jpg] [ni10107f2.jpg] [ni10107t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}