 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 58, No. 3, May-June, 2010, pp. 424-428 Original Article Significance and cost-effectiveness of somatosensory evoked potential monitoring in cervical spine surgery Chakib Ayoub1, Tony Zreik2, Raja Sawaya3, Nathalie Domloj4, Amira Sabbagh4, Ghassan Skaf4 1 Department of Anesthesiology, American University of Beirut Medical Center, Beirut, Lebanon Date of Acceptance: 24-Nov-2009 Code Number: ni10108 PMID: 20644272 Abstract
Background : Intraoperative somatosensory evoked potential (SSEP) monitoring during cervical spine surgery is not a universally accepted standard of care. Our retrospective study evaluated the efficacy and cost-effectiveness of intraoperative SSEP in a single surgeon's practice. Keywords: Cervical spine surgery, healthcare costs, somatosensory evoked potential monitoring Introduction Maintenance of the functional integrity of the spinal cord is the main concern of every surgeon treating patients with cervical spine disease. Risks arise from unintentional trauma, traction, compressive or ischemic injury to the spinal cord. Recently, there has been a growing emphasis on the use of intraoperative neurophysiological monitoring in an attempt to detect dysfunction of the nervous tissue at a stage during which it is still reversible. [1] Intraoperative somatosensory evoked potential (SSEP) monitoring has been evaluated in neurovascular, [1],[2] skull base [3],[4],[5] and spine surgery. [6],[7],[8] Although intraoperative SSEP monitoring has been routinely used during lumbar and thoracic spine surgery, [9] its recent use in cervical spine surgery has been found to be sensitive in detecting neurological insult caused by mechanical stress, surgical manipulation, hypotension and ischemia. [10],[11],[12] Review of the literature failed to show the significance and cost-effectiveness of intraoperative SSEP routine monitoring in cervical spine surgery. We studied intraoperative SSEP monitoring during 210 consecutive cervical spine procedures performed by a single surgeon. The purpose of this retrospective study is to correlate the intraoperative SSEP monitoring efficacy with the postoperative neurological status of the patient and to scientifically assess the cost-effectiveness of this procedure in cervical spine surgery. Materials and Methods This study is based on a retrospective review of 210 consecutive cervical spine surgeries performed by the same surgeon in a tertiary care center from July 1999 till June 2005. The average patient age was 50.4±16.2 years with 147 males. SSEP monitoring was used in all these surgeries. The medical records of the 210 patients were reviewed after obtaining consent from the Institutional Review Board at the American University of Beirut Medical Center. The data collected included: age, gender, preexisting medical co-morbidities, smoking status, preoperative neurological deficit, SSEP findings, surgical technique, postoperative neurological status and complications. A standardized anesthesia protocol was adopted to reduce the impact of anesthetics on SSEP recording. Patients were induced with propofol 1-2 mg/kg, cisatrecurium 1-3 μm/kg/min and maintained with fentanyl 1 mcg/kg/h, supplemented with isoflurane 0.5% air and oxygen. Routine monitoring was done, including arterial line. Anesthesia was maintained constant with a mean blood pressure of 55 mm Hg. Normocarbia and normothermia were maintained. Intraoperative SSEP monitoring was performed in 140 patients treated by an anterior cervical approach and in 70 patients treated by a posterior approach. Preoperative diagnoses included cervical disc disease with radiculopathy (95 patients), cervical spondylosis with radiculopathy and/or myelopathy (68 patients), cervical spinal fractures with myelopathy (22 patients), and cervical spinal tumor with myelopathy (25 patients), with the latter including schwannomas (11 patients), meningiomas (4 patients), ependymomas (3 patients), and astrocytomas (7 patients). Cervical myelopathy was evident clinically in 115 patients. The most frequently treated level was C 5 -C 6 disc accounting for 53% of the patients. Univariate and multivariate logistic regression analysis, student's t test, and χ2 tests with version 14.0 of SPSS were used for statistical analysis. P<0.05 was considered to be the level of statistical significance. Technique of SSEP monitoring Intraoperative SSEP monitoring was performed in all 210 surgeries as described previously. The monitoring started after the induction of anesthesia and throughout the entire surgery. SSEPs were measured using the Nicolet Viking IV apparatus. The posterior tibial nerves were stimulated at the medial malleolus of each foot alternatively. Recordings were done Cz' at the cortex and at the popliteal fossa by needle electrode. The reference electrode was placed at Fz, and the ground electrode at the forehead. Stimulation was started prior to general anesthesia and the positioning of the patient. The level of stimulation was increased until the toes started contracting. This level was maintained throughout the surgery. The stimulus duration was 0.3 milliseconds, and its frequency 5 Hz. High pass filter was 3 KHz. Low pass filter was 10 Hz. Average responses appeared on the screen after 300 averagings, around once per min. The stimulation of both posterior tibial nerves was uninterrupted during the induction of anesthesia, positioning of the patient, and throughout the different stages of the surgery. The latency of the popliteal and cortical responses, as well as the amplitudes were monitored and stored. The anesthesiologist was instructed to inform the electrophysiologist upon any change in anesthesia or administration of any medication. New baselines were considered adjusted to the changes in anesthesia regimen or patient variables. Indirect monitoring of motor function is common with intraoperative SSEP monitoring, but significant change in motor evoked potiental (MEP), despite normal SSEP, has been reported. [13] When a spinal shock occurs in the ventral part of the spinal cord, there could also be a transient worsening of the intraoperative SSEP monitoring. The surgeon was informed by the electrophysiologist, upon a 50% drop in amplitude or a 10% increase in the latency of the baseline cortical waves. The surgeon responded to these changes by interrupting the surgery and observing the persistence of the changes or the return to baseline. Several changes in the cortical and the popliteal waves may be observed during these procedures:
Cost analysis To evaluate the cost-effectiveness of using SSEP in cervical spine surgery, several calculations were established:
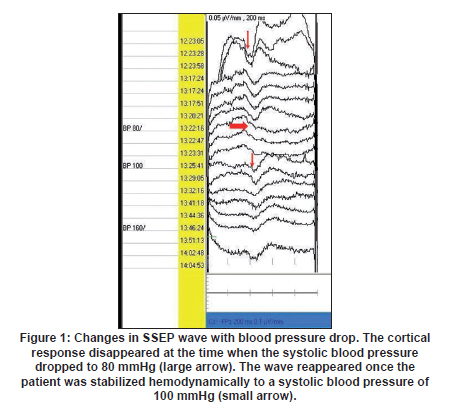
Acute Care Medical Costs + (Annual Lifetime Care Costs ΄ Pt Life Expectancy)= Total Lifetime Medical Costs These findings were compared to several recent studies that evaluated the economic impact of medical care, rehabilitation and life support services for a spinal cord injury survivor. The financial information of all 210 patients was analyzed in conjunction with the University Medical Center Business Office. Results The majority (45%) of patients presented with cervical disc disease. The mean hospital stay was 6±4 days. The patients' diagnoses and indications for surgery are outlined in the methodology section. During the 210 cervical spine procedures, temporary loss of the wave during cauterization occurred in the majority of cases; however, discontinuation of the cautery resumed the baseline SSEP wave. We had no cases of loss of the cortical wave with preservation of the popliteal wave. In one patient, a drop in the amplitude of the cortical wave by > 50% and a delay in the latency by >10% occurred, secondary to a drop in the systolic blood pressure by 25-30 mm Hg; the baseline SSEP characteristics reappeared after hemodynamic stabilization of the patient, and no neurological deficits occurred. In addition, a drop in the SSEP amplitude by 40-50% and a delay in the amplitude by 10% occurred in two cases during the surgical procedure [Figure - 1]. The surgeon was notified intraoperatively of these changes. In one case the response returned to the normal baseline after interrupting the surgery and waiting for few min for the abnormality to defuse. The wave remained stable thereafter. In the second case, the drop in amplitude and delay in latency returned as soon as the surgeon resumed surgery on the cord (readjustment of bone graft). The cortical waves returned to baseline and persisted uninterrupted until the end of the surgery. Cost analysis Total cost without monitoring - Total direct cost with monitoring The average cost of the hospital stay (including surgery) for the cases without postoperative neurological deficits was $13,000. The total cost of a SSEP monitoring unit with trolley and computer screen, in addition to a staff neurophysiologist is estimated to be $31,564 per year. The total estimated cost per patient is $595, assuming 53 patients per year. This cost is in accordance with a recent study, conducted at the McGill Health Center, which estimated the cost per case for SSEP monitoring to be $463. [15] A German study found a cost per case of 196.40 Euros (US$=261). [16] An analysis at the Mayo Clinic in the United States assumed the cost per case to be US$570. [17] The neurologist consultation is estimated to be $50 per patient. The operation time was increased by 1 h compared to a procedure without monitoring, with an estimated additional cost of approximately $40. The total intravenous anesthesia is predicted to cost 20% more than the usual anesthesia, approximately $150. The additional amount in dollars for SSEP monitoring arrived to $835 per patient. In conclusion, the total cost of the surgery with monitoring amounts to $13,835. Total cost with postoperative injury Based on records of previous cases that sustained neurological deficit following surgery, the average cost of the hospital stay for the cases with postoperative neurological deficits was 30,000$. However, one should also take into account the costs of healthcare after discharge from hospital in addition to the indirect cost that might include job loss for instance. According to recent data on spinal cord injury, annual medical costs for health and human services, durable goods and expendable commodities were calculated for different age groups. The annual medical costs were $95,638.92 for ages 20 to 35; $109,462.66 for ages 35 to 55 and $133,756.66 for ages 55 and onward. [18] The life expectancy of a quadriplegic patient is expected to be 30 years post injury. [19] Based on reported results in the literature, [9],[10] the incidence of postoperative deficits, in the absence of monitoring, is estimated in 3% of patients, with 20% of these deficits (0.6% of all patients) expected to be permanent. At our Center, 0.6% represents 1 of the 210 patients. The institution would be saving a total cost ranging from $64,074.92 to $102,192.66 for each patient injured per year. This health benefit would be achieved at a total cost, to the institution, of approximately $31, 564 per year. Discussion In order to estimate the cost-effectiveness of SSEP monitoring, we calculated the total cost of SSEP monitoring for 100 patients in our center and compared it to the total medical costs for health and human services in addition to durable goods and expendable commodities for one patient (1% of cases) injured for a total of 30 years. SSEP monitoring amounted to $59,500 for the 100 patients. If a postoperative deficit occurs in 1% of cases or to say one case of the 100 cases monitored, the total medical costs for health and human services in addition to durable goods and expendable commodities is estimated to be $2,869, 167.6 for age 20 to 35; $3,283,879.8 for age 35 to 55 and $4,012,699.8 for age 55 and continuing for the 30 year-survival. SSEP monitoring is a useful adjunct in the surgical management of cranial base tumors and is a good predictor of postoperative neurological function. [3] A correlation between intraoperative SSEP deterioration and postoperative outcome has been described in previous reports. [20],[21] In contrast, the occurrence of a postoperative motor deficit without an associated change in SSEPs can be attributed to anterior spinal artery syndrome or direct injury of the ventral spinal cord. [22] This seems to be less relevant for "orthopedic indications" of spinal surgery but essential for "neurosurgical indications" with intramedullary involvement. Nuwer et al., [23] reported a false positive rate for intraoperative SSEP monitoring of 0.063% in scoliosis surgery whereas Legatt et al., [13] demonstrated a significant change in MEP intraoperative monitoring despite normal SSEP monitoring. Several investigators have used intraoperative monitoring with SSEPs. Epstein et al,[10] were among the first to establish the efficacy of SSEP monitoring for cervical spine surgery. The results of 218 unmonitored patients were compared to the results of 100 monitored patients. In the unmonitored group, eight patients became quadriplegic and one patient died. In the monitored group, neither quadriplegia nor death occurred, but there was one technical error. May et al., [24] used SSEP in 191 surgical procedures involving the cervical spine. The cortical SSEPs were found to be reliable for monitoring the cervical spinal cord especially during complex surgeries. The technique was also sensitive and in the authors' view the "false positives" encountered may indicate a high rate of preventable incidents. Kombos et al., [25] studied the impact of SSEP monitoring on anterior cervical surgery, where intraoperative SSEP monitoring was performed in 100 patients treated by an anterior cervical approach. It was concluded that intraoperative SSEP monitoring was easy to perform and helped in increasing safety during anterior cervical surgery. The results of the present study add to a small but growing body of literature that points to the value of intraoperative neurophysiological monitoring of SSEPs during cervical spine surgery. It seems that SSEP is quite effective and cost-effective when used during cervical spine surgery. Continuous SSEP monitoring is an easy and practical tool that helps increase safety during anterior cervical spinal cord surgery. Our results illustrate the potential utility of intraoperative monitoring during cervical spine surgery. In a study conducted on demographics of spinal cord injury (SCI) between 1942 and 1997, the most obvious trends were a greater percentage of SCI due to medical and surgical causes and falls and smaller percentage due to motor vehicle accident. Surgical causes accounted for 6.7%, and medical reasons for 6.8%. [26] The reduction of neurological deficit was attributed in part to early SSEP detection of vascular or mechanical compromise to the spinal cord or nerve roots and to the immediate alteration of anesthetic or surgical technique in response to somatosensory-evoked potential changes, i.e., reversal of systemic or "relative" hypotension, adjustment of operative position, release of distraction, and cessation of manipulation. Conclusion Intraoperative SSEP monitoring, in our surgical population, proved to be a reliable method for preventing postoperative neurological deficit by the early detection of vascular or mechanical compromise, and the immediate alteration of the anesthetic or surgical technique. Moreover, it was found to be cost-effective since our tertiary care center saves a total cost ranging from $64,074 to $102,192 per patient injured per year for an additional expense of $31,546 per year on SSEP monitoring. References
Copyright 2010 - Neurology India The following images related to this document are available:Photo images[ni10108f1.jpg] |
| |||||||||

{kind=link}