 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
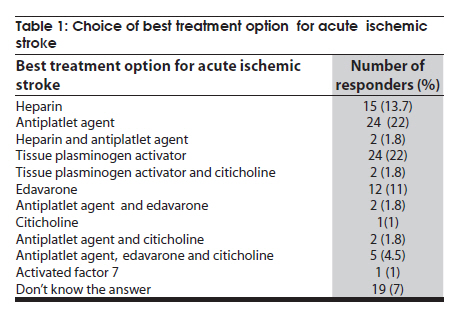
Neurology India, Vol. 58, No. 3, May-June, 2010, pp. 441-442 Brief Report Treatment of acute ischemic stroke: Awareness among general practitioners S Aaron, M Alexander, T Maya, V Mathew, M Goyal Neurology Unit, Department of Neurological Sciences, Christian Medical College, Vellore, Tamil Nadu, India Date of Acceptance: 08-Jan-2010 Code Number: ni10111 PMID: 20644275 Abstract For promptly referral of a patient with acute ischemic stroke (AIS) for possible thrombolysis, general practitioners (GPs) need to equipped with the advanced knowledge of AIS treatment. We assessed the knowledge regarding treatment of AIS among GPs practicing in and around a quaternary care teaching hospital in south India. A total of 109 GPs who attend to medical emergencies were interviewed using a standard questionnaire. Of the 109 GPs interviewed, 54% felt that tissue plasminogen activator (tPA) can be used in the treating AIS, but only 24% had chosen tPA as the best treatment option and 22% opted for other agents like citicholine or edavarone. Only 17% were aware that tPA should be given within 3 h. and 35% felt that intra-arterial thrombolysis as a treatment option.. Only 30% felt the need for good sugar control and 37% wanted aggressive lowering of blood pressure. Majority of GPs are not clear about beneficial effects of thrombolysis and are not updated regarding BP and sugar control in the setting of AIS. Keywords: Acute ischemic stroke, general practitioners, thrombolysis Introduction Intravenous tissue plasminogen activator (tPA) is the recommended treatment in acute ischemic stroke. [1] The barriers for thrombolysis treatment in the Indian context include: (1) delayed arrival at the hospitals because of lack of awareness about the signs of stroke [2],[3] and also available therapeutic options among the population; (2) lack of enough centers offering thrombolysis; (3) economic affordability; and (4) lack of awareness about stroke thrombolysis among the medical professional. We studied the awareness about treatment of AIS among general practitioners (GPs). Materials and Methods The study was conducted within a radius of 40 km from a quaternary care teaching hospital in south India, where thrombolysis (both intravenous and intra-arterial) is being offered routinely to patients with AIS. The neurology department had initiated an acute stroke awareness program as a first step while starting an acute stroke network. A total of seven continuing medical education (CME) programs on "management of ischemic stroke: the first 12 hours" were held in the nearby secondary level hospitals for the local GPs who had at least a MBBS degree. All of them handle medical emergencies including acute strokes. A questionnaire was designed containing basic questions on AIS management. Before the CME program, all the participants were asked to fill the questionnaire. While analyzing. questionnaire filled by the GPs were separated from the questionnaire filled by other health care workers. The data was compiled and analyzed using Microsoft Office Excel 2003. Results A total of 109 GPs completed the questionnaire and the responses included: Q 1: Opinion about tPA in the management of AIS: Of the 109 GPs, 59 (54%) agreed that tPA can be used in the treatment of AIS; 30 (28%) were not aware of this drug; ten (11%) thought that tPA is a drug undergoing clinical trial and nine (8%) felt that tPA has no role in the treatment of AIS. Q 2: The best treatment option for a patient with AIS: (See [Table - 1] - choice of best treatment option for acute ischemic stroke) only 26 (24% of total study -cohort) felt tPA as the best possible treatment option. Thirty five GPs (32%), felt an antiplatelet agent alone or in combination with a neuroprotective agent or heparin as the best treatment option and 24 (22%) GPs opted for a neuroprotective agent either citicholine or edavarone. Q 3: Window period for tPA: Only 19 (17%) GPs were aware that tPA needs to be given within 3 h of onset of stroke;. 47 (43%) did not know when to give this drug; 11 (10%) felt it can be given up to 12 h; 24 (22%) felt it can be given within the first 6 h;, and 8 (7%) felt it should be given within the first 1 h. Q 4: Intra-arterial thrombolytic therapy for AIS: Regarding intra-arterial thrombolytic therapy, 39 (35%) felt it was a useful treatment option; 31 (28%) were not aware of such procedure; 9 (8%) felt that it has no role, and 30 (27.5%) thought that it has only been tried in clinical trials. Q 5: Blood pressure (BP) control in AIS: In a patient with AIS and high blood pressures: of the 109 GPs, 51 (47%) felt that the BP should be lowered - systolic < 185 mmHg and diastolic < 110 mmHg; five (4.5%) felt that the systolic < 200 mmHg and diastolic < 130 mmHg would suffice; 32 (29%) felt that the BP to be lowered to normal with systolic 120 mmHg and diastolic 80 mmHg; 9 (8%) wanted the BP to be reduced below normal with systolic <120 mmHg and diastolic <80 mmHg; and 12 (11%) were not sure of what should be the ideal BP in the setting of AIS. Q 6: Blood sugar control in AIS: For a patient with AIS and a blood sugar of 289 mg/dL: of the 109 GPs, 48 (44%) felt that the high sugar need not be treated; 33 (30%) felt that insulin should be started to get the sugar below 200 mg%; 9 (8%) opted for oral hypoglycemic agents; and 19 (17%) responders were not sure of the management. Q 7: Intravenous fluids in AIS: If intravenous fluids are required for a patient with AIS, of the 109 GPs, 29 (26%) opted for dextrose, 33 (30%) for saline, 30 (27.5%) for ringer lactate, and 17 (15%) were not sure. Discussion The first likely medical contact for patients with AIS will be a local medical practitioner. It is very important that the first medical contact is aware of the various treatment options available for the patient and also the nearest center providing such treatment options for prompt referral. In this survey only 24% of the GPs opted for tPA as the best treatment for a patient with AIS. Only 17% were aware that tPA needs to be given within the first 3 h. Thus in this region of the country only one out of four potentially treatable case of AIS will be referred promptly for possible thrombolytic therapy. In a German study, [4] two-thirds of the GPs would immediately admit stroke-suspected patients. A study in England [5] had shown that visiting a GP can significantly delay patient arrival at the hospital. Knowledge regarding blood pressure management and control of sugars in the setting of AIS was inadequate. Of the GPs surveyed, 37% wanted aggressive lowering of the BP which can be potentially harmful. [6] High sugars can have detrimental effects in acute brain injury of all types.In this study 30% practicing physicians felt the need about aggressive management of hyperglycemia and need to avoid glucose-containing solutions. It is also striking that 22% of the GPs chose aggressively marketed drugs like edavarone and citicoline over tPA. This study has some limitations. This study had sampled GPs only form a small geographic area and hence the results cannot be generalized. However, the results of this study suggest that there is an urgent need to update the knowledge regarding treatment of AIS among GPs in the country. Following this study, we have set up a 24-h acute stroke hotline. Any GPs in this region when receives a patient with acute stroke can call and clarify points regarding referral for thrombolysis or clear any doubts regarding acute conservative treatment. References
Copyright 2010 - Neurology India The following images related to this document are available:Photo images[ni10111t1.jpg] |
| |||||||||

{kind=link}