 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
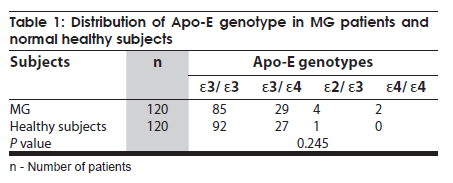
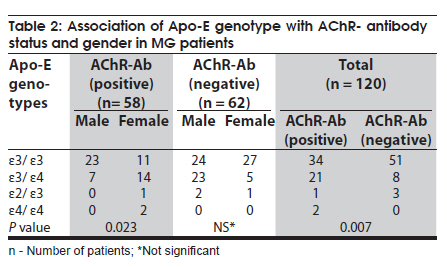
Neurology India, Vol. 58, No. 3, May-June, 2010, pp. 443-445 Brief Report Apolipoprotein-E genotypes and myasthenia gravis Hamid Suhail1, Christhunesa C Soundararajan1, Subbiah Vivekanandhan2, Sumit Singh1, Madhuri Behari1 1 Department of Neurology, All India Institute of Medical Sciences, New Delhi, India Date of Acceptance: 01-Feb-2010 Code Number: ni10112 PMID: 20644276 Abstract Autoimmune myasthenia gravis (MG) is a disorder of neuromuscular junction. Possible role of multiple genes in the development of the MG has been documented. This case-control study, studied the association of apolipoprotein E (Apo-E) alleles with MG. Anti-AChR antibody was measured using radio receptor immunoassay. Apo-E genotypes were analyzed in 120 MG patients and 120 healthy subjects. Comparison between patients with MG and controls showed no significant association with Apo-E allelic variants. However, a significant association of Apo-E4 allele with AChR-antibody positive patients was observed (P = 0.007). Also, among seropositive patients, a significant association was seen between female gender and Apo-E4 allele (P = 0.023). Our results suggest that the presence of Apo-E4 allele might influence seropositive status in patients with MG and seems an associated susceptible factor in female patients. Keywords: AChR, Apolipoprotein-E, autoimmunity, myasthenia gravis, genotype Introduction Apolipoprtein-E (APO-E) polymorphism is one of the most extensively studied polymorphism in different ethnic groups worldwide. Apo-E allele frequencies vary from population to population. Apo-E gene is located on chromosome 19q13.2 and consists of 299 amino acids with a molecular weight of 34 KDa. [1] It exists in three distinct isoforms: Apo-E2, Apo-E3 and Apo-E4, due to interchanges of cysteine- arginine at 112 and 158 codon positions. [2] ApoE3 is the most common form of allele and it is found in more than half of the population. Apo-E is the major apolipoprotein in the central nervous system (CNS) [3] where it is synthesized by glia, macrophages and neurons. [4] It is also found in the peripheral nervous system (PNS) where it is produced by nonmylinating Schwann cells, ganglionic satellite cells and macrophages. [5] Apo-E is attributed to influence risk and severity of several CNS) and PNS disorders. Possession of Apo-E4 is associated with an increased risk of Alzheimer's disease (AD). It is also reported that Apo-E4 is associated with chronic progressive decline in multiple sclerosis. There is also evidence that Apo-E4 increases the risk of peripheral neuropathy in human immunodeficiency virus (HIV) infection and diabetic mellitus. [6] An increased frequency of Apo-E4 allele in inclusion body myositis compared with that in patients with other inflammatory disease has been reported. [7] The presence of Apo-E4 confers increased risk of disease and worse prognosis, while the presence of Apo-E2 confers a decreased risk of disease and a better prognosis. [8] Acquired myasthenia gravis (MG) is an autoimmune disorder of neuromuscular junction characterized by fatigable muscle weakness and presence of antibodies against nicotine acetylcholine receptors (nAChR-Abs) in majority of cases. Apo-E has a role in the modulation and synthesis of T- lymphocytes. [7] T-lymphocytes play a significant role in the immunopathogenesis of autoimmune MG. Apo-E alleles also influence the integrity of skeletal muscles. Apo-E4 allele are believed to facilitate deposition of β amyloid fragments in skeletal muscle leading to muscle cell degeneration.[7] These findings and loss of cholinergic receptors in synaptic cleft in MG, prompted us to study the association between MG and Apo-E genotypes. Materials and Methods Samples The study subjects consisted of 120 patients with MG (male: female = 59: 61) undergoing treatment in neurology outpatient clinic of a tertiary referral center in north India and 120 controls matched by age, sex and ethnicity. Of the 250 patients with MG enrolled over two years period from 2004 to 2006, 120 patients (mean age of onset 36.8 ± 17.7 years) (range 4-72 years) were chosen randomly after obtaining written informed consent. Seventy-seven patients had mild disease (I+IIA) and 43 patients had moderate to severe (IIB+III+IV) disease. All patients had fulfilled the established diagnostic criteria for MG. These include predominant proximal muscle weakness, fatigability improving with rest and worsening with exertion, repetitive nerve stimulation test (RNST) showing > 10% decrement response suggestive of a post synaptic neuromuscular junction (PSNMJ) disorder and good response to tensilon/neostigmin test. [9] The study protocol was approved by the institute ethics committee. Antibodies assays Serum AChR-Abs levels were measured in duplicate in all the patients by standard radioimmunoassay (RIA) methods, using radio receptor assay kit [IBL Immuno Biological Laboratories Hamburg, Germany] as per the manufacturer's protocol . Acetylcholine receptor from human muscle was used as antigen in this radio receptor assay. The receptors were labeled with 125 I-alpha-bungarotoxin ( 125 I-a-BgT). Values ≥ 0.4 nmol/L were considered positive. [10] Antibodies were immunoprecipitated, centrifuged and pellets were washed twice with wash buffer and counted per minute in a gamma counter. The frequency of positivity for AChR-Abs among patients with MG in our setup is 60% (personal data), which is much lower than that reported for Caucasian and Oriental populations (80- 85%). [11] DNA isolation and Apo - E genotyping DNA was isolated from peripheral blood leukocytes following conventional phenol/chloroform methods. A portion of the Apo-E gene was amplified by polymerase chain reaction (PCR) using the primers TCC AAG GAG CTG CAG GCG GCG CA (forward) and TCG CGG GCC CCG GCC TGG TAC ACT GCC (reverse), following a step-down protocol. Along with the regular PCR ingredients, 7% dimethyl sulfoxide (DMSO) was also added. The annealing temperature for the step-down PCR started with 65 o C for one minute with a decrease of 0.5 o C per cycle for the first 20 cycles and the final annealing was done at 55 0 C for the next 15 cycles. The PCR products (224-bp) were digested with HhaI restriction enzyme and resolved by 15% polyacrylamide gel electrophoresis (PAGE) for determining the genotype based on band pattern published previously. [12] Statistical Analysis Chi square (χ2 ) test was used to measure the significant difference between the patients with MG and controls. A 'P' value of ≤ 0.05 was considered as significant. All the statistical analysis was carried out using SPSS 11.5 statistical package. Results Different Apo-E genotypes found in patients with MG and controls are given in [Table - 1]. The most frequent allele found was Apo-E3. The allele frequencies of Apo-E found in control subjects were E3 = 0.883, E4 = 0.113 and E2 = 0.004 and they were in accordance to Hardy-Weinberg equilibrium based on the genotypic frequencies calculated (χ2 = 0.417, df = 2, P = 0.879). Chi-square analysis of Apo-E allelic and genotypic frequencies between patients and controls showed no significant association. A comparison within the MG group on AChR-antibody status showed that Apo-E4 allele had a significant association with the positivity of AChR antibody (χ2 = 12.11, df = 3, P = 0.007) status [Table - 2]. No association was observed between Apo-E allele and gender, both in the patients and controls. However, within the MG group, a statistical significance was seen (P = 0.023) between female gender and Apo-E4 allele among AChR-antibody positive cases. Discussion The allelic and genotypic analysis in our study does not show a strong association of Apo-E genotypes with MG. In an earlier study by Sostarko et al. [13] an association was found between E2/E4 genotypes (46.43%) and patients with MG, but none with E4/E4 genotype. Contrary to this, we found E4/E4 genotypes in two (3.45%) seropositive patients, but none of the patients, both seropositive and seronegative, and control subjects had E2/E4 genotypes. The study by Sostarko et al. [13] had also shown an association between severe form of MG (32.14%) and Apo-E2/E4 genotypes. This is not the case in our study (data not given). Also, when the allelic frequencies were compared within the patients with MG, we found a significant association of Apo-E4 allele among the seropositive patients. The interaction between Apo-E4 allele and loss of nicotinic acetylcholine receptors (nAChRs) in AD remains controversial. [14] Our finding of significant association of Apo-E4 allele among the seropositive patients indicates the possible role of E4 allele in MG, as has been hypothesized in patients with AD. However, the presence of Apo-E4 allele influencing the positivity of AChR- antibody status in patients with MG is not clear. Although the role of Apo-E has been implicated in the process of nerve regeneration and repair and in smooth muscle proliferation and differentiation; its role in skeletal muscle metabolism has not yet been clearly defined. [15] Apo-E is also involved in the modulation of T-lymphocytes activation by mitogens or antigens. [15] Higher frequency of Apo-E4 genotype has been reported in patients with diabetes mellitus and severe neuropathy compared to other genotypes. [16] It may be conjectural to hypothesize that Apo-E4 allele by modulating T-cells influence antibody formation against AChRs. Though, in general we did not observe any significant association between gender and Apo-E allelic variants, a significant association of Apo-E4 allele within female seropositive patients was observed. From the above results, it is possible to say that an association between Apo-E4 allele with seropositive status of MG might trigger the antibody against the AChRs in MG. Apo-E4 allele appears more at risk in female patients than male patients. This is the first report on association of specific Apo-E allele with AChR-antibody status in patients with MG in Indian population. This observation needs to be strengthened by conducting a similar study using a larger sample size. Acknowledgments The financial grant for the study was supported from Indian Council of Medical Research (ICMR), New Delhi, India, is gratefully acknowledged. We also thank ICMR for supporting the Senior Research Fellow who worked in this study. References
Copyright 2010 - Neurology India The following images related to this document are available:Photo images[ni10112t1.jpg] [ni10112t2.jpg] |
| |||||||||

{kind=link}
{kind=link}