 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
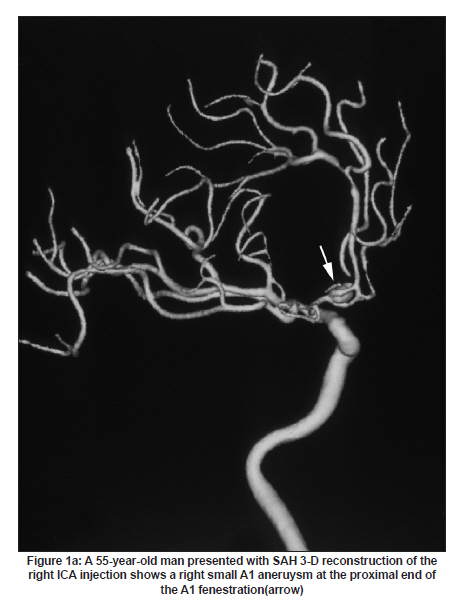
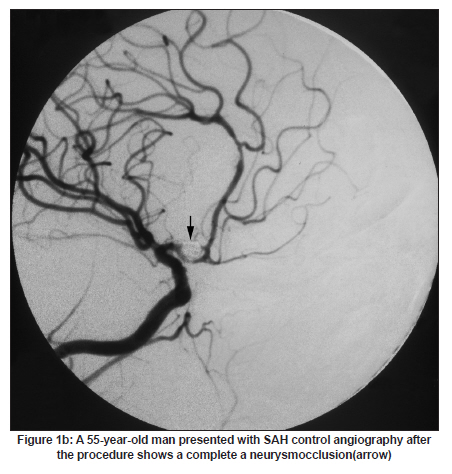
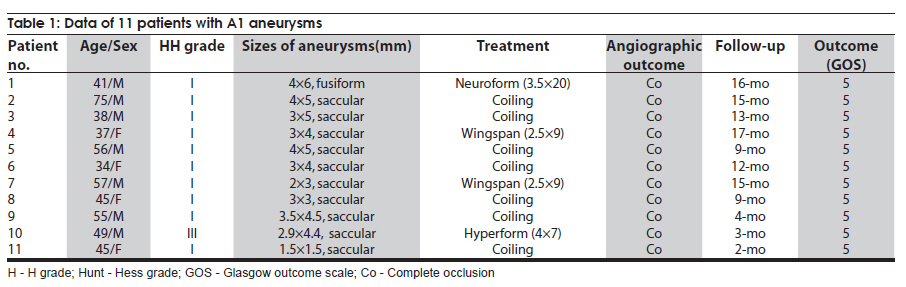
Neurology India, Vol. 58, No. 3, May-June, 2010, pp. 446-448 Brief Report Endovascular treatment of A1 segment aneurysms of the anterior cerebral artery Bo Yu1, Zhongxue Wu2, Xianli Lv2, Yunhui Liu1, Meng Sang1 1 Department of Neurosurgery, Shengjing Hospital of China Medical University, Shenyang, Liaoning, China Date of Acceptance: 08-Jun-2010 Code Number: ni10113 PMID: 20644277 Abstract Aneurysms of the A1 segment of the anterior cerebral artery (ACA) are rare and challenging to treat. We evaluated our experience of endovascular treatment in 11 patients with A1 segment aneurysms of ACA. Seven aneurysms were treated with coiling; three were treated with stent-assisted coiling and one was treated with balloon-assited coiling. Endovascular treatments were technically successful and without complication. Follow-up examinations showed complete cure in all 11 patients. Keywords: Anterior cerebral artery, endovascular treatment, intracranial aneurysms Introduction Aneurysms of the A1 segment of the anterior cerebral artery (ACA) represent less than 1% of all intracranial aneurysms but are important cause of nontraumatic subarachnoid hemorrhage (SAH). [1],[2],[3],[4],[5],[6],[7],[8],[9] Most of these aneurysms are treated by either surgical or endovascular treatment because of the high associated risk of bleeding. [1],[2],[4],[7],[9] There is limited data in the literature concerning the endovascular treatment of A1 segment of ACA. [6],[10] The aim of this study was to report our experience with endovascular treatment and imaging follow-up of 11 patients with A1 aneurysms of ACA. Patients and Methods From January 2007 to December 2009, 1012 patients with 1054 aneurysms were treated in our institution; 11 (1.1%) of them had an A1 segment aneurysms. All the A1 aneurysms were ruptured and indication for treatment was subarachnoid hemorrhage (SAH). The Hunt and Hess grades were 1 in 10 patients and 3 in 1 patient and all were Fischer grade 2 or 3. The size of the aneurysms varied from 1.5 to 6 mm (mean 4.1 mm) and 3 aneurysms had a branch at the neck. Eight aneurysms were superiorly located, a few millimeters after the internal carotid artery (ICA) bifurcation. Endovascular treatment was performed in all the patients. All patients were treated by endosaccular coiling. An Echelon-10 microcatheter (M.T.I-ev3, CA, USA) was used in all patients [Figure - 1a and Figure - 1b]. If stent-assisted coiling was required, patients were put on 75 mg clopidogrel and 200 mg aspirin for at least 3 days before the endovascular procedure and were maintained on the same dosage for at least 4 weeks. Aspirin was continued indefinitely. Aneurysm obliteration was evaluated by angiography. Clinical outcome was graded according to a modified Glasgow Outcome Scale (GOS). [11] Patient follow-up angiography was performed at 3-10 months. Further examinations were obtained yearly if needed. Results Eleven patients with A1 segment aneurysms were treated during the study period, and the results are shown in [Table - 1]. There were seven men and four women, the mean age was 48.4 years (range 34-75). The maximum dimension of the sac ranged from 1.5 to 6 mm (mean 4.10.9 mm) and aneurysm neck size ranged from 0.8 to 4 mm (mean 1.80.8 mm). Of the 11 aneurysms, seven (63.6%) were narrow-necked and four (36.4%) were wide-necked. The perforating artery was incorporated into the neck in three (27.3%). These aneurysms were treated at choronic stage of SAH, because these patients were referred to our center from local hospitals. Endovascular treatment was successful in all the patients. The stent was also used to protect perforator and parent artery in three patients. The microcatheter was navigated into the aneurysm before stent placement. One Neuroform (Boston Scientific, CA, USA) and two Wingspan (Boston Scientific) stents were used. No technical complication occurred in our patients. Heparin was maintained for 48 h, aspirin (200 mg/day) and clopidogrel (75mg/day) was administered for 6 months if a stent was used. There were no silent, infarctions on post-operative CT scans. All patients showed an excellent clinical outcome (GOS=5). Immediate angiographic control showed a complete occlusion in all cases. Follow-up angiogram was obtained in all the patients and showed complete occlusion. Discussion A1 segment aneurysms of ACA have been diagnosed with increasing frequency probably because of increasing awareness. [6] Our results demonstrate that treatment is indicated for all of these lesions. Natural history of spontaneous rupture has been documented in the literature [1],[3],[7],[9] and was seen in all of our patients. Three-demesion angiography are essential for the diagnosis of these lesions. Treatment can be chosen after assessing location and configuration of the aneurysm, adjacent branches, collateral circulation, and time of presentation. Our study shows that endovascular treatment of A1 aneurysms is feasible and associated with good clinical and anatomical results. The A1 aneurysm catheterization is challenging because of its small size and its superior location. [6] In these cases, the microcatheter could not safely be placed or stabilized. And because of their location, small size, and close relationship with perforators, endovascular treatment frequently requires the use of stent. [12],[13],[14],[15],[16],[17],[18] Aneurysms of the proximal ACA have three characteristics that differ from intracranial aneurysms in general: [2],[7],[9] (1) they are usually small; (2) they can arise at the origin of perforators; and (3) they are rupturing at smaller size. Because of these specific features, A1 aneurysms are technically challenging to treat. [6] There is limited data on the neurosurgical and endovascular treatment. [1],[2],[3],[4] However, in our institution, most A1 aneurysms were treated by endovascular approach. The challenging part of endovascular treatment is aneurysm catheterization because they are small and superiorly located, a few millimeters after ICA bifurcation: [6],[19] in this situation, the microcatheter guidewire is inferiorly directed to enter A1 origin and, then, it must immediately be turned in the opposite direction to enter the aneurysm. This maneuver is stressful, risky, and sometimes impossible. In order to safely catheterize A1 aneurysms, the microcatheter tip should be shaped in "S". This shape matches the anatomical structure of ICA bifurcation and A1 segment and facilitates aneurysm catheterization, stabilize the microcatheter, and decrease the risks in case of perforation. If a stent is needed and the aneurysm is small, we usually navigate a microcatheter priorly to stent deployment. The stent can stabilize the microcatheter, eliminate protrusion of coils and protect perforator at the neck. [18] In our experience, these adjunctive techniques were mandatory to treat most of the A1 aneurysms. Despite the frequent use of these techniques, none of out patients had any post-procedural neurological deficits, highlighting the safety of endovascular treatment. Moreover, anatomical results were satisfying and stable in all the followed up patients. Therefore, our series suggests that endovascular treatment can be proposed as an alternative therapeutic option for the management of A1 aneurysms. The follow-up results in this series were rather for a short follow-up time, and longer follow-up would be needed to see the long term effect of the treatment. References
Copyright 2010 - Neurology India The following images related to this document are available:Photo images[ni10113t1.jpg] [ni10113f1b.jpg] [ni10113f1a.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}