 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
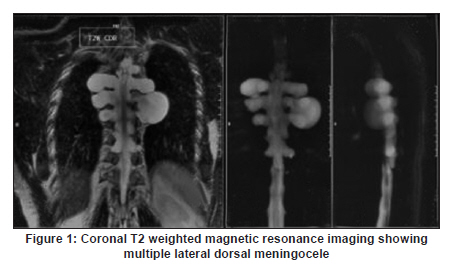
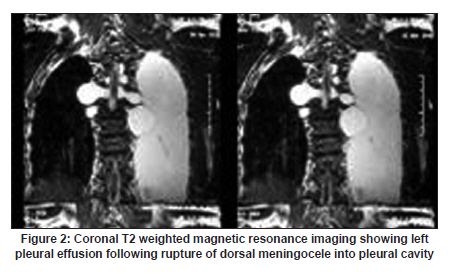
Neurology India, Vol. 58, No. 3, May-June, 2010, pp. 466-467 Case Report Spontaneous subarachnoid pleural fistula: A rare complication of lateral thoracic meningocele Vimal Kumar, Yashpal Singh Bundela, Vikas Gupta, Sanjeev Dua, Anil Kumar Singh Division of Neurosurgegry, Department of Neurosciences, Fortis Hospital, Sector 62, Noida, Uttar Pradesh, India Date of Acceptance: 08-Jun-2010 Code Number: ni10118 PMID: 20644282 Abstract A case of spontaneous subarachnoid pleural fistula following rupture of a thoracic meningocele into the pleural cavity is described in this article. The patient had symptoms of low-pressure headache and difficulty in breathing. The fistulous opening was closed near the foramina by rotating a vascularized muscle flap. After showing initial improvement the patient had a recurrence of symptoms after 6 weeks, with a small leak at the closure site. A lumbar thecoperitoneal shunt led to permanent cure. In this article we discuss the course of the disease, the symptoms, the diagnostic methods, and the various treatment modalities for subarachnoid pleural fistula. Keywords: CSF fistula, ruptured meningocele, spontaneous subarachnoid pleural fistula, subarachnoid pleural fistula Introduction Subarachnoid pleural fistula is a rare entity with varied clinical presentations and poses a diagnostic challenge. [1] We report an unusual case of spontaneous subarachnoid pleural fistula following rupture of a lateral thoracic meningocele into the pleural cavity. A male aged 58 years presented with complaints of headache in the upright position, with vomiting and progressive respiratory difficulty of 2 months duration. His chest X-ray showed right side pleural effusion and bilateral multiple radiolucent lesions. Magnetic resonance imaging (MRI) of the chest confirmed that these lesions to be a lateral meningocele [Figure - 1], [Figure - 2], [Figure - 3]. The pleural cavity was tapped and the fluid, analysis was consistent with cerebrospinal fluid (CSF) [Figure - 2]. Intraoperatively, rupture of a meningocele into the pleural cavity was confirmed and the sac was closed just outside the foramina. After isolating the nerves, the closure was reinforced with a vascularized muscle flap. A minute leak 6 weeks later led to recurrence of symptoms, which responded well to CSF diversion via a thecoperitoneal shunt. Till date only 54 cases of subarachnoid pleural fistula have been reported. The first case reported was by Millory in 1959. [2] Most of the reported cases occurred following trauma to a local malignant lesion. [3],[4],[5] Spontaneous subarchnoid pleural fistula is extremely rare and only one such case secondary to cystic degeneration of a neurofibroma has been described. [6] The fistulous tract, once formed, remains patent due to the positive subarachnoid pressure and the negative intrapleural pressure. Clinical features are either related to excessive CSF drainage from the subarachnoid space or related to obliteration of the pleural cavity. [1] Rarely, it can cause meningitis or pneumocephlus or it may be an incidental finding. In the present patient there were multiple lateral thoracic meningoceles, probably congenital in origin, and rupture of one of the meningoceles had led to the fistula and the associated clinical symptoms. Probably this may be the first case of such nature. The treatment options vary from simple observation to complex operative procedures. However, all symptomatic patients require treatment. A relatively simple method of treatment is chest tube drainage with positive pressure ventilation. However, this is effective only in traumatic fistulas. [7],[8] In spontaneous and malignant fistulas, unhealthy tissues around the tract prevent spontaneous closure thus necessitating direct obliteration. [9] Obliteration of the tract requires laminectomy, thoracotomy, or a paraspinal approach. Local vascularized intercostal muscles are the best interposition grafts. A small-output fistula may respond to CSF diversion procedures. References
Copyright 2010 - Neurology India The following images related to this document are available:Photo images[ni10118f1.jpg] [ni10118f3.jpg] [ni10118f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}