 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
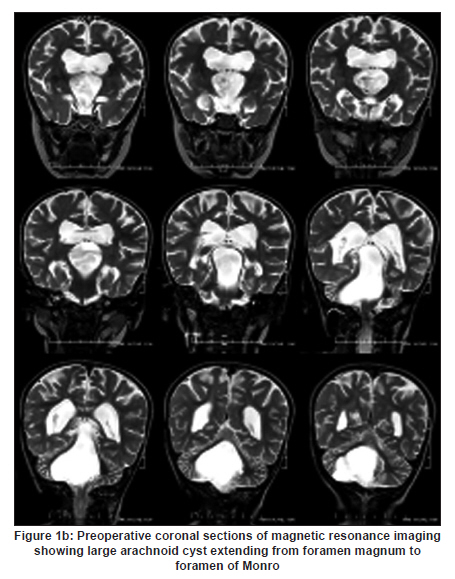
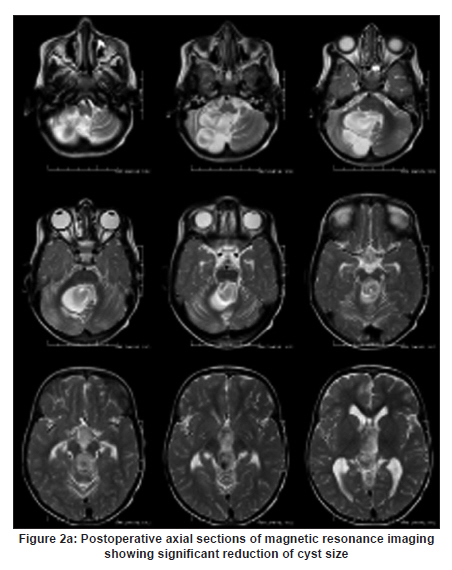
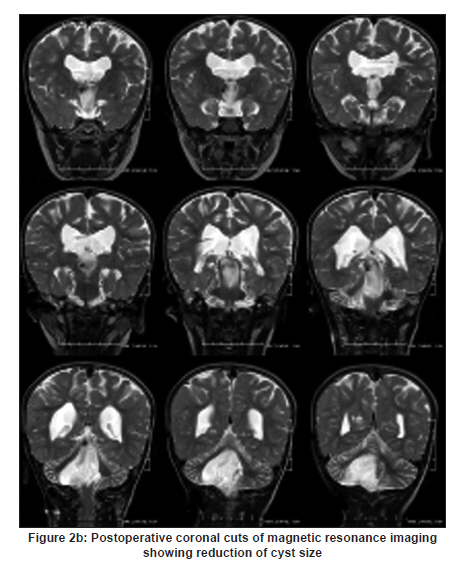
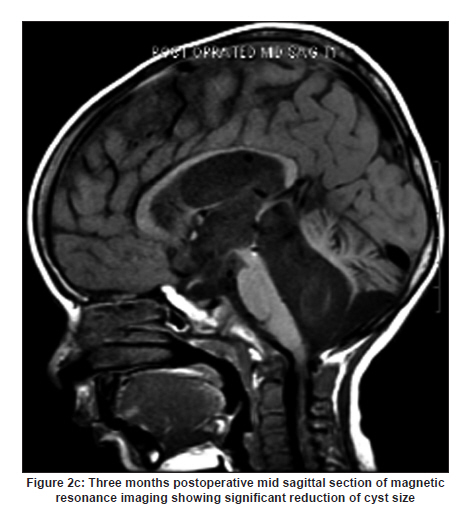
Neurology India, Vol. 58, No. 3, May-June, 2010, pp. 481-484 Case Report Endoscopic management of large multicompartmental intraventricular arachnoid cyst extending from foramen magnum to foramen of Monro YR Yadav1, Abhijeet Basoor2, Mina Todorov3, Vijay Parihar1 1 Department of Neurosurgery, NSCB Medical College, Jabalpur, Madhya Pradesh, India Date of Acceptance: 08-Jun-2010 Code Number: ni10122 PMID: 20644286 Abstract The treatment options for symptomatic arachnoid cysts are shunting, open craniotomy, and endoscopic fenestration. Endoscopic fenestration of large arachnoid cyst is safe and effective. Postoperative subdural hematoma and intraparenchymal hemorrhage can be avoided by endoscopic fenestration. This technique has the additional advantage of identifying and treating ventricular abnormalities, such as foramen of Monro stenosis and cerebral aqueduct occlusion. This report describes endoscopic dual fenestration in a child with large multicompartmental intraventricular arachnoid cyst extending from foramen magnum to foramen of Monro. The child presented with difficulty to hold the neck in upright position, irritability, vomiting, and large head. Follow-up postoperative magnetic resonance imaging at 3 months showed a significant reduction in size of the cyst. Clinically, the patient showed a gradual improvement at 10 months follow-up. Probably this is the first report of this nature. Keywords: Arachnoid cysts, central nervous system cysts, endoscopy, hydrocephalus, nervous system malformations Introduction Arachnoid cyst can be managed by shunt, [1] craniotomy with fenestration, [2] or endoscopic treatment. [3],[4] Both shunting procedures [1] and craniotomy with fenestration [2],[5] have limitations, and endoscopic treatment of arachnoid cyst has been found to be safe and effective. [6],[7] There is only a single case report of multicompartmental cysts. [8] This report describes endoscopic treatment and management of a large intraventricular cyst occupying multiple compartments. Case Report A 3-year-old male presented with inability to hold his neck upright, irritability, and vomiting. Past history was significant for ventriculo-peritoneal shunt done at another facility at the age of 18 months with no improvement. Neonatal history was unremarkable. On examination, there was spontaneous eye opening and movement of all the four limbs equally. Head circumference was 59 cm. Magnetic resonance imaging (MRI) of the brain showed a cystic lesion extending from foramen magnum to foramen of Monro passing through the fourth ventricle, aqueduct of sylvius, and third ventricle [Figure - 1a, Figure - 1b and Figure - 1c]. An endoscopic fenestration was performed. Postoperative MRI showed a slight reduction in the cyst size without evidence of any intracranial hematoma or effusion. There were no postoperative complications. Histopathologic examination of the cyst wall was suggestive of arachnoid cyst. The patient showed a gradual improvement and was discharged on postoperative day 7. Three months postoperatively, MRI showed a significant reduction in the size of the cyst [Figure - 2a, Figure - 2b and Figure - 2c]. On follow-up at 10 months, the child experienced no further vomiting, was able to hold his head up, and could accept oral feeds. He could sit and walk with support and also play. A right-sided burr hole was made, 2 cm anterior to coronal suture. The lateral ventricle was hit free hand. The foramen of Monro was identified at the confluence of choroid plexus, thalamostriate vein, and septal vein. The arachnoid cyst was protruding through the foramen of Monro and obstructing it. The vessels on the cyst wall were coagulated by bipolar forceps. Dual openings were made in the cyst wall. One opening of more than 1 cm was made in the superior cyst wall, which opened into the right lateral ventricle. An endoscope was introduced into the cyst. Fenestration of more than 1 cm was made in the inferior cyst wall on the floor of the third ventricle. The infundibular recess and mammillary bodies were not clearly seen on the floor of the third ventricle. Dorsum sellae was recognized by gentle probing with bipolar forceps. Third ventriculostomy of about 6 mm was carefully made just posterior to dorsum sellae. The cyst was communicating superiorly with the lateral ventricle and inferiorly with the interpeduncular cistern. There was no evidence of infection or hemorrhage in the cyst wall or ventricular margins. Coagulation shrinkage of the superior cyst wall was done. A 30° angled scope was used for inspection after making the fenestrations in the cyst wall. Poorly visualized optic chiasma was pushed anterosuperiorly. The cyst was finally communicating superiorly in the third ventricle and inferiorly in the cistern. Discussion Arachnoid cysts are frequent incidental findings on neuroimaging studies. The exact origin of these cysts is not clear. Four possible theories have been proposed: (i) Ball valve mechanism theory suggests a possible anatomic communication between the cyst and the subarachnoid space, which acts as a one-way valve resulting in the cyst enlargement. The observation of cerebrospinal fluid (CSF) flow through a slit-like valve during the endoscopic procedure by Schroeder and Gaab [9] gives some evidence to this theory; (ii) Osmotic gradient theory suggests a gradient-driven fluid transport between subarachnoid space and cyst. However, great compositional similarities between CSF and the cyst fluid content do not support this theory; (iii) Developmental malformation theory suggests that arachnoid cyst is a trapped fluid content in cerebral lobe agenesis; and (iv) Hypersecretion theory suggests excess fluid production by cells lining the luminal cyst wall. There is morphologic and ultrastructural evidence to support the secretory nature of the cyst wall. Ultrastructurally, the cells lining the cyst demonstrate the presence of microvilli on the luminal surface and cytoplasmic vesicles that are consistent with fluid secretion. Moreover, enzyme immunocytochemistry demonstrated sodium-potassium adenosine triphosphatase in the plasma membranes lining the cavity at the luminal side and near the intercellular clefts at the basolateral side, a structural organization consistent with fluid transport toward the lumen. The argument against continuous secretion is based on the fact that cysts often remain static in size and sometimes disappear, thus suggesting that secretion is neither universal nor likely the only mechanism involved. Aquaporins (AQP1) have been found to support the hypersecretion theory. [10] The presence of ectopic choroid plexus in the arachnoid cyst was given as a cause for the expansion of the cyst. [11] It has been proposed that arterial pulsation on the cyst wall can also result in the enlargement of the cyst. [3] Nakamura and colleagues [3] observed strong pulsation of the cyst wall at the foramen magnum synchronous with the pulsation of the left vertebral artery and no pulsations of the cyst wall over the remaining portions of the brain. Schroeder and Gaab [9] observed pulsations of the cyst wall around the vertebral artery during an endoscopic procedure. Peraud and colleagues [8] also reported rapid development of arachnoid cyst and proposed valve-like mechanism, vessel pulsation on one part of the cyst, and hypersecretion as possible mechanisms of cyst enlargement. The cyst in our patient seems to have developed in early intrauterine life and enlarged to a big size. The possible mechanism of cyst growth in our patient could have been a result of valve-like mechanism and vessel pulsation on one part of the cyst. Another mechanism could be hypersecretion by cyst lining. The arachnoid cyst could rupture spontaneously producing symptomatic subdural effusion or hematoma (SDH) in previously asymptomatic patients. There could be a spontaneous disappearance of the cyst or it could remain constant in size for a long period of time. The optimal treatment for symptomatic arachnoid cysts remains controversial. Some of the options include cyst shunting, open craniotomy, and endoscopic fenestration, each procedure with its own risks. The chance of SDH after craniotomy is approximately 4% and the risk is higher with a large arachnoid cyst. [2] Craniotomy can result in life-threatening intraparenchymal hemorrhage. Decompression of arachnoid cysts can also result in total impairment of brain function by interfering with cerebral perfusion. [5] Although the pathophysiology of postoperative hematoma is unclear, it could be due to re-perfusion injury, abrupt changes in blood circulation, faulty autoregulation, and superficial vein distortion by brain decompression. [5] It has been suggested that more gradual decompression of arachnoid cysts using indirect surgical approaches with programmable shunts or more conservative procedures, such as simple tapping, may decrease the incidence of such complications. [1],[12] Endoscopic technique can avoid such rare but serious complications associated with sudden decompression after craniotomy. [5] Postoperative subdural fluid collection, which is not uncommon after craniotomy treatment of cyst underlying dura mater, can be avoided by endoscopic fenestration via a transcortical approach. [13] Endoscopic fenestration is a minimally invasive technique and is considered to be the treatment of choice in symptomatic arachnoid cyst. [3] Ventricular abnormalities, such as stenosis of the foramen of Monro and cerebral aqueduct occlusion contributing to hydrocephalus, may be associated with arachnoid cysts. Endoscopic exploration of the cyst has an additional advantage of identification and treatment of such ventricular abnormalities. [4] Dual endoscopic fenestration into the intraventricular compartment and basal cistern is safe and effective compared with single fenestration. [7] Neuronavigation can help in the proper placement of cyst fenestration. [6] It has been suggested that endoscopic fenestration and coagulation shrinkage of suprasellar arachnoid cysts aid in preventing blockage of aqueduct by cyst wall. [14] Cyst-peritoneal shunt is another treatment. This too has complications, such as shunt dependency, shunt infection, over drainage, and shunt blocks. [1] References
Copyright 2010 - Neurology India The following images related to this document are available:Photo images[ni10122f1a.jpg] [ni10122f3.jpg] [ni10122f1b.jpg] [ni10122f2c.jpg] [ni10122f2a.jpg] [ni10122f2b.jpg] [ni10122f1c.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}