 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
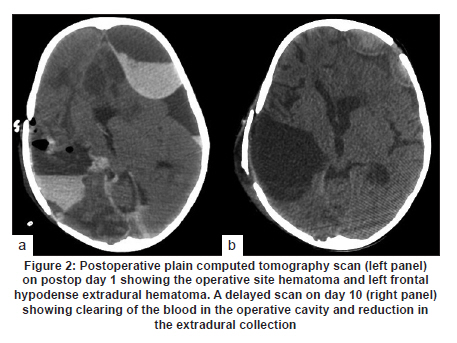
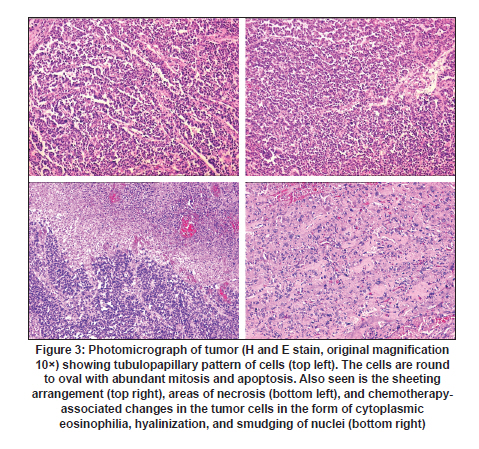
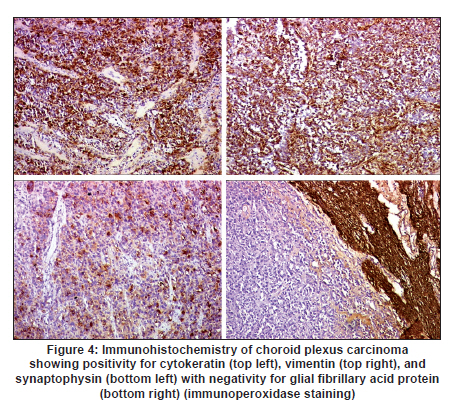
Neurology India, Vol. 58, No. 3, May-June, 2010, pp. 485-486 Letter To Editor Hyperacute disseminated intravascular coagulation following surgery for a choroid plexus carcinoma in a child Aliasgar V Moiyadi1, Rakesh Jalali2, Santosh Menon3 1 Neurosurgical Services, Department of Surgical Oncology, Tata Memorial Centre, Mumbai, India Date of Acceptance: 08-Jun-2010 Code Number: ni10123 PMID: 20644287 Sir, A 5-year-old boy presented with progressive left-sided weakness and mental obtundation. Two-and-a-half years before this admission, he had surgery elsewhere for a presumed primitive neuroectodermal tumor followed by radiotherapy and chemotherapy. At presentation, he was drowsy and was responsive to repeated calls. He had a dilated, unreactive right pupil and left hemiparesis. A contrast-enhanced computed tomography (CT) scan showed a large isodense enhancing mass in the right fronto-temporo-parietal lobe with severe edema and uncal herniation [Figure - 1]. Preoperative blood counts, biochemical investigations, and a coagulation profile were normal and he was taken up for emergency surgery. Total excision of the large, well-delineated, vascular, lobulated mass of variegated consistency was done. Intraoperatively just after the debulking was commenced, he developed hematuria. Repeat coagulation profile showed a reduction in the platelet count and fibrinogen level along with prolonged prothrombin time as well as activated partial thromboplastin time (aPTT/PTTK) [Table - 1]. The blood loss till then was around 150 mL (overall 1200 mL). Blood gases were normal and euthermia was maintained throughout the procedure. Adequate blood volume, fresh frozen plasma, cryoprecipitate and platelet concentrate were administered. There was no intraoperative hemodynamic instability. Mismatched blood transfusion was also ruled out. Postoperatively the coagulopathy persisted and fibrin degradation products were elevated, suggesting a disseminated intravascular coagulation (DIC) along with secondary hyperfibrinolysis. Postoperative CT scan showed an operative site hematoma and a contralateral frontal biconvex collection of mixed density suggestive of extradural hematoma [Figure - 2]. Under cover of platelets and fresh frozen plasma, the partially clotted hematoma was evacuated. Over the next few days, the coagulopathy reverted [Table - 1] and he slowly improved neurologically. At discharge on postoperative day 14 he was opening eyes, obeying simple commands, and had residual grade 4 left hemiparesis. Histology [Figure - 3] and immunohistochemistry [Figure - 4] confirmed the tumor to be a choroid plexus carcinoma. Unfortunately, we were unable to procure the previous slides for review. A hypercoagulable state has been described in certain brain tumor types, such as malignant gliomas and meningiomas, predisposing the individual to thromboembolic complications. Although less frequent, a hypocoagulable state with a hemorrhagic diathesis is probably as important, if not more. [1],[2] Current understanding suggests that most of these cases are due to a hyperfibrinolytic state either primary or secondary to disseminated intravascular coagulation (DIC). DIC results from the release of tissue thromboplastin from brain/tumor triggering the intrinsic pathway of coagulation and may produce a hyperfibrinolytic state, though not always. A primary hyperfibrinolytic state can also be seen in certain cases due to release of tissue plasminogen activator (t-PA) by certain tissues, such as the meninges and choroid plexus. [3] Variable coagulation defects have been described in children undergoing choroid plexus tumor surgeries, [4] however, frank DIC is unusual. [4],[5] The clinical picture along with the laboratory findings (low levels of fibrinogen, elevated levels of fibrin degradation products, and less number of platelets) in our patient confirmed a diagnosis of DIC with secondary hyperfibrinolysis. [6] Its rapid occurrence early during surgery was the interesting aspect and took us by surprise. The clinical implications of a hemorrhagic disorder in a brain tumor patient are significant. Postoperative hematomas are a major concern and can be very challenging. The clinical course of events may unfurl rather rapidly. Hence a high index of suspicion and prompt intervention are essential. Monitoring of the coagulation system parameters using routine and special testing has been suggested to preempt and correct potentially fatal complications. [2] The treatment of DIC has to be tailored according to the cause, severity, and spectrum of manifestations. The underlying cause needs to be addressed and reversed. Supportive care along with replacement of coagulation factors and platelets with plasma, cryoprecipitate, and factor concentrates is advocated. Although surgical intervention is risky, it can be performed under cover of an appropriate therapy. The benefit of such a calculated risk was borne out by our case. References
Copyright 2010 - Neurology India The following images related to this document are available:Photo images[ni10123t1.jpg] [ni10123f4.jpg] [ni10123f2.jpg] [ni10123f1.jpg] [ni10123f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}