 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
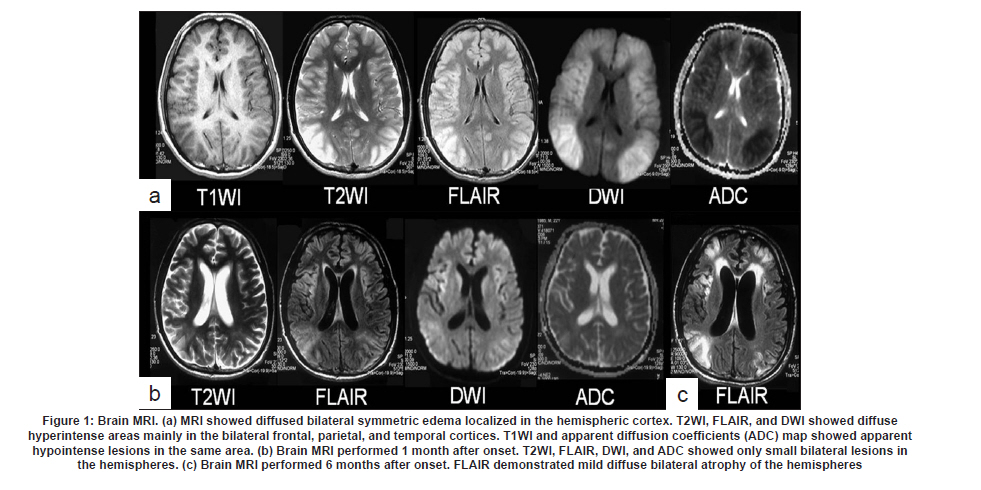
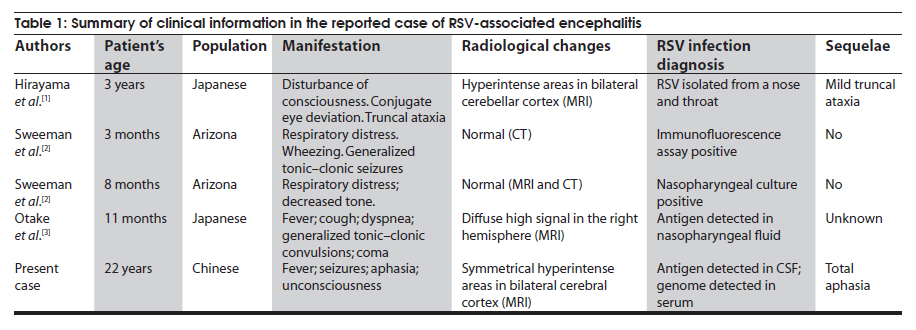
Neurology India, Vol. 58, No. 3, May-June, 2010, pp. 489-490 Letter To Editor Respiratory syncytial virus encephalitis with symmetrical bilateral hemispheric lesions in an adult Fu Bo Cheng1, Yan Hua Li1, Gui Hua Jin1, Kang Ding Liu1, Yan Bo Sun2, Wei Wu1, Jia Chun Feng1 1 Department of Neurology, The First Affiliated Hospital of Jilin University, Changchun - 130021, China Date of Acceptance: 03-Nov-2009 Code Number: ni10126 PMID: 20644290 Sir, Respiratory syncytial virus (RSV) usually causes respiratory diseases and RSV-associated encephalitis is very rare. [1] RSV-associated encephalitis has been reported more in pediatric patients, and is relatively more common in Japanese children. [1],[2],[3] There are fewer reports of RSV-associated encephalitis in adults. [4],[5] Here we report a rare adult case of RSV encephalitis, with diffuse bilateral symmetric lesions in the cerebral cortex. A previously healthy 22-year-old male was admitted with fever, seizures and loss of consciousness. Direct and indirect papillary light reflexes were normal. Deep tendon reflexes were brisk and plantar response was bilaterally up going. There was no neck stiffness. The white blood cell count was 22 300/mm 3 . All other investigations were normal. Brain computed tomography (CT) scan on the first day after onset was normal. Lumbar puncture, the opening pressure was 200 mm H 2 O. Cerebral spinal fluid (CSF) analysis: cells: 120 leukocytes/ml (86% lymphocytes); protein: 218 mg/l and glucose: 3.9 mmol/l; normal myelin basic protein (MBP) and oligoclonal IgG band. Anti-RSV IgM antibody in the CSF had a 2.01 cutoff index. The RSV genome was detected in the serum by reverse transcriptase- polymerase chain reactions (RT-PCR) technique. Tests for other viral infections were negative. Electroencephalography (EEG) on the second day of onset showed diffuse high-voltage slow waves. The auditory brainstem response was normal. Brain magnetic resonance imaging (MRI) showed diffuse lesions in the bilateral frontal, parietal, and temporal cortices, with swelling of the cerebral cortex and narrowing of the cerebral fissures [Figure - 1]a. Patient was treated with dexamethasone and ribavirin. He recovered consciousness three weeks after the onset of illness. Brain MRI, performed 1 month after onset, showed disappearance of the lesions seen in the first MRI [Figure - 1]b. Six months after onset, MRI demonstrated mild diffuse bilateral atrophy in the hemispheres [Figure - 1]c. At one year follow-up still patient continues to have total aphasia. Most of the reports of RSV-associated encephalopathy have been from the Japan in pediatric population [1],[2],[3],[6] [Table - 1] There are few reports of RSV-associated encephalopathy in adults. [4],[5] Neurologic sequelae can occur. [1],[2] EEG has been found to be a sensitive investigation to detect neurological abnormalities in patients with RSV infection. [7] In our case, the brain MRI changes showed an interesting feature: the diffuse lesions predominated in the bilateral frontal, parietal, and temporal cortices. Acute disseminated encephalomyelitis (ADEM) is an unlikely explanation for this patient's illness, because the lesions of ADME are predominately located in the peripheral subcortical cerebral white matter. [8] The pathologic mechanism underlying RSV encephalitis is still unknown. Using single-photon emission tomography (SPECT), some researchers have shown hypoperfusion and hypometabolism in the gray matter, suggesting possible neuronal damage, which might explain the persistence of neurological sequelae even after several years. [1],[3] Our case is rare in that there was bilateral symmetric hemispheric involvement. Miura et al. [9] have also reported a case of symmetrical brainstem encephalitis caused by herpes simplex virus. Our case and the case reported by Miura et al. [9] does not support the hypotheses of brain asymmetry immunological system evoked in some others reports. [10],[11] Acknowledgments The authors thank Drs Lorna Grant and William Orr, University of Manitoba, Canada, for their critical reading of the manuscript and suggestions for improving the English. References
Copyright 2010 - Neurology India The following images related to this document are available:Photo images[ni10126f1.jpg] [ni10126t1.jpg] |
| |||||||||


{kind=link}
{kind=link}