 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
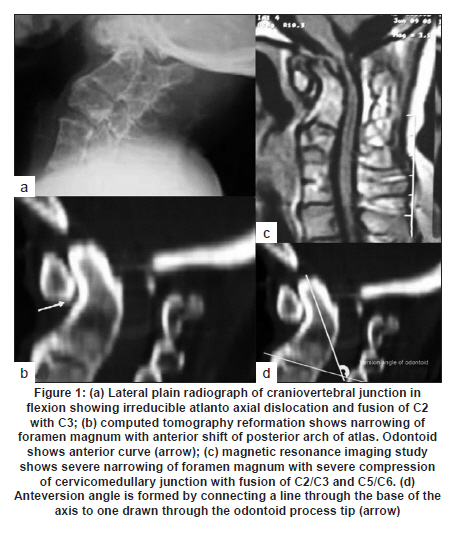
Neurology India, Vol. 58, No. 3, May-June, 2010, pp. 490-492 Letter To Editor Anteverted odontoid: A rare congenital bony anomaly of craniovertebral junction Mudumba Vijayasaradhi, Gurram L Phaniraj, B.L.S. Kumar Department of Neurosurgery, Nizam's Institute of Medical Sciences, Hyderabad, Andhra Pradesh - 500 482, India Date of Acceptance: 08-Jun-2010 Code Number: ni10127 PMID: 20644291 Sir, The most common anomaly of the odontoid process is the os odontoideum, but there is also a spectrum of variations ranging from hypoplasia to complete aplasia. [1],[2],[3] Anteverted odontoid process is rare, and the exact embryologic factor or anomaly leading to its occurrence is unknown. A 41-year-old woman presented with progressive weakness of all the limbs and also stiffness of limbs of 3 years duration. On examination, she had gross restriction of neck movements and clinical signs suggestive of high cervical compressive myelopathy at the craniovertebral junction. Radiographs of the cervical spine showed hypoplasia of the atlantic ring, an anteriorly curved odontoid process with a fixed atlantoaxial dislocation, and blocked C2-C3 and C6-C7 vertebrae [Figure - 1]a. These findings were confirmed with a computed tomography scan [Figure - 1]b Magnetic resonance imaging showed severe cord compression with myelomalacia changes in the cord [Figure - 1]c. On imaging, the compressing structure was the junction of the body of C2 with odontoid, but not the tip of odontoid. The patient was taken up for surgery and first she underwent transoral decompression followed by C1 posterior arch excision and occipitocervical fusion. Postoperatively the patient recovered well and fusion was noted at 6 months of follow-up. Several anomalies have been described with respect to the odontoid process, such as the os odontoideum, posteriorly inclined odontoid, os terminale, odontoid hypoplasia, aplasia, and odontoid duplication. [5],[6],[7],[8],[9] All these anomalies occur as a result of maldevelopment or abnormal migration of ossification centers. In this patient with anteverted odontoid and normally developed axis (C2), we hypothesize that this anomaly would have resulted from the traction by the apical ligament over the tip of the odontoid process during the early developmental stages of craniovertebral junction during which period the apical ligament is thick and active. In humans, the apical ligament is considered rudimentary and indeed shows little increase in its size in adults as compared with its initial size in fetuses. [9] A review of the literature suggests no report of a case of anteriorly curved odontoid process over the body of C2 vertebra. Anteversion angle is the angle formed by connecting a line through the base of the axis to the line drawn through the tip of the odontoid process. [10] In the same study, the measured normal retroversion of the odontoid in controls was mean 95° and range 60-105° [11] In the present case, the angle of retroversion was 136°, which is a very rare feature. [Figure - 1]d. Probably, the anterior curvature of the odontoid could have led to neural compression at a later age than expected, that is, after 40 years of age rather than in the childhood. With regard to the association of Klippel-Feil anomaly, various associated anomalies of the odontoid process have been described, such as odontoid hypoplasia, superior migration of odontoid, os odontoid, and atlantoaxial instability. [12],[13],[14] In present case, there is no evidene of the Klippel-Feil anomaly in association with anteverted odontoid as in some cases reported in the literature. Anteversion of odontoid is the angulation anomaly seen at the synchondrosis of C2 body and odontoid process. As the anteversion angle increases, there is an increased chance of cord compression by the body of axis (the offending element) rather than the tip of the odontoid. Management guidelines of this anomaly remains the same as that of any other craniovertebral junction anomaly, namely, decompression of the offending body portion followed by occipitocervical fusion. [1],[15] References
Copyright 2010 - Neurology India The following images related to this document are available:Photo images[ni10127f1.jpg] |
| |||||||||

{kind=link}