 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
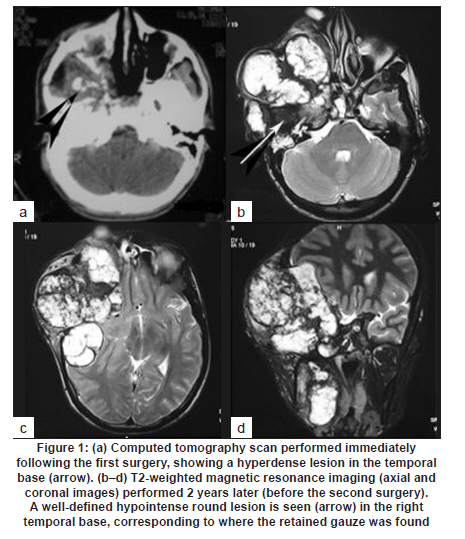
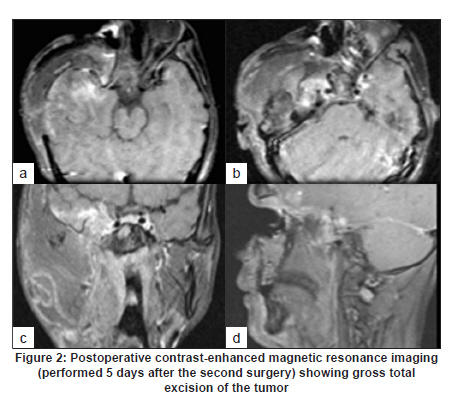
Neurology India, Vol. 58, No. 3, May-June, 2010, pp. 492-493 Letter To Editor Intracranial gossypiboma: An under-reported entity Aliasgar V Moiyadi1, Prathamesh Pai2, Pankaj Chaturvedi2, Anil D«SQ»Cruz2 1 Department of Surgical Oncology, Neurosurgical Services, Tata Memorial Hospital, Parel, Mumbai, India Date of Acceptance: 12-Oct-2009 Code Number: ni10128 PMID: 20644292 Sir, A 23-year-old man presented to us with a recurrent skull base chondrosarcoma (having undergone surgery elsewhere 2 years ago). He had a large swelling in the right temporal region extending into the lateral orbit (producing proptosis) and involving the ipsilateral maxilla and mandible. He was blind in the right eye and had right-sided fifth nerve palsy (since the time of first surgery). Magnetic resonance imaging (MRI) revealed a large tumor of heterogenous intensity [Figure - 1]b-d involving the right temporal bone extending into the infratemporal fossa, orbit, maxilla and the ipsilateral mandible with intracranial extension into the middle cranial fossa. A uniformly hypointense (on T1- as well as T2-weighted MR images) well-rounded lesion in the temporal base was noted, which retrospectively was realized to be the gauze piece. We acknowledge that in view of the extent and heterogeneity of the lesion, we did not consider this possibility preoperatively. On subsequent review of the computed tomography (CT) scan performed immediately following the first surgery in 2004, a well-defined hyperdense mass in the same area [Figure - 1]a could be appreciated. We performed an anterolateral craniofacial resection with a free anterolateral thigh flap reconstruction. At surgery, the temporal pole appeared gliotic and a well-defined mass measuring 2 cm in diameter was seen within the parenchyma. When separated and delivered out, it was clearly seen to be a rolled-up gauze piece covered with blood clots. There was no suppuration. No intradural tumor was identified. The postoperative recovery was smooth, except for transient cerebrospinal fluid leak (rhinorrhoea), which responded to drainage lumbar punctures. The postoperative MRI showed no residue [Figure - 2]. The final histopathology was a recurrent chondrosarcoma and he was subsequently referred for adjuvant radiotherapy. Gossypibomas are often an embarrassment for most surgeons. Although reported in general surgical literature, [1],[2] gossypibomas in the neurosurgical setting are extremely uncommon, most probably due to under-reporting. A review in 2001 found only seven articles addressing this topic in the neurosurgical literature. [3] Although most of the cases reviewed had no adverse consequences due to the retained material, the authors warned of the potential complications and medicolegal implications of such accidents. Retained gauze pieces following spinal surgeries are known. [3],[4] Few other cases of "muslinomas" secondary to intentional wrapping of aneurysms [5],[6] and gossypibomas secondary to resorbable hemostatic agents [7] have also been reported. Intracranial-retained gauze is extremely rare, if not unreported. Although the previous surgery in our patient was performed elsewhere and the operating surgeons were not available for discussion, the most likely scenario would have been (given the location of the lesion and proximity to the pterygoid plexus and cavernous sinus) torrential intraoperative bleeding necessitating packing with gauze. The blood-covered gauze may have then been overlooked during the closure leading to its retention and gossypiboma formation. The CT and MRI appearance of retained gauze/cotton is highly variable, depending on the time period following surgery when it is imaged. [8] A centrally hyperintense lesion on T2-weighted MR images surrounded by a rim of hypointensity is the most commonly reported finding. A central wavy or spotted pattern is also suggestive of a gauze piece. [4] However, any well-defined mass at the operative site, in the absence of blood, should always be looked upon suspiciously. In the presence of recurrent tumor, the finding may be missed. This happened in our case too, although retrospectively, we realized that the uniformly hypointense area was distinctly different from the rest of the tumor imaging morphology and that its location corresponded to the site of the retained gauze intraoperatively. Most gossypibomas in the neurosurgical patient remain clinically silent. [3] However, the potential to elicit a foreign body reaction and subsequent mass effect cannot be overlooked, as also the risk of suppuration with fatal complications. A cautious and unhurried approach during surgery is mandated to prevent such occurrences, especially in long and emergency surgeries. [1] Careful counting of all gauze pieces and use of tailed cotton/gauze would help eliminate such accidents. Meticulous inspection of the wound before closure should be routine and not left to juniors assisting the surgery. When intentionally left behind, it should be clearly documented to avoid confusion in interpreting postoperative scans. References
Copyright 2010 - Neurology India The following images related to this document are available:Photo images[ni10128f1.jpg] [ni10128f2.jpg] |
| |||||||||


{kind=link}
{kind=link}